
Introduction: The objective of the present study is to evaluate the impact of extended pelvic resection on abdominoperineal amputation for low rectal cancer.
Methods: A retrospective study was conducted with patients with low rectal adenocarcinoma who underwent abdominoperineal resection in a single center between 2020-2023. Patients were divided into two groups: conventional abdominoperineal resection (APR) and extended abdominoperineal resection (APRe). APR associated with the resection of adjacent organs due to direct tumor invasion were considered extended pelvic resections, including hysterectomy, cystectomy, prostatectomy, and colpectomy. The outcomes evaluated were complications (graded according to the Clavien-Dindo classification), reoperation, readmission, length of hospital stay, surgical time, blood transfusion, number of lymph nodes retrieved, surgical margins, disease-free survival, and overall survival.
Results: 32 patients with low rectal adenocarcinoma who underwent abdominoperineal resection (16 APR and 16 APRe) were included, with a mean age of 58 years (±13) and female predominance (66%). All patients were treated with neoadjuvant chemotherapy and radiotherapy. Age, sex, American Society of Anaesthesiologists physical status (ASA), pre-treatment oncologic staging, and surgical approach were similar between groups (p>0.05). The surgical time (405 ± 101 vs. 339.9 ± 56.5 minutes; p=0.034) and the number of blood units transfused (1.25 ± 1.61 vs. 0.25±0.58 units; p=0.031) were higher in the APRe group. Disease-free survival was worse in the APRe group (HR: 8.15 ± 5.42; p=0.002). There was no significant difference in overall survival (HR: 3.72 ± 2.84; p=0.085). There was no significant difference for intraoperative complications (12.5 vs. 37.5%; p=0.22), postoperative complications (56.3 vs. 43.8%; p=0.724), and serious complications (31.3 vs. 31.3%; p>0.999). There was also no difference in reoperation rate (31.3 vs. 18.8%; p=0.343), length of hospital stay (13.53 ± 17.4 vs. 9.85±12.6 days; p=0.564), readmission (31.3 vs. 37.5%; p>0.999), compromised margins (25 vs. 12%; p=0.654), and number of lymph nodes retrieved (21.25 ± 7.8 vs. 19.31 ± 10.7 lymph nodes; p=0.564).
Conclusion: Extended abdominoperineal amputation is associated with a greater risk of bleeding and longer operative time. The need for extended resections implies a worse long-term prognosis.
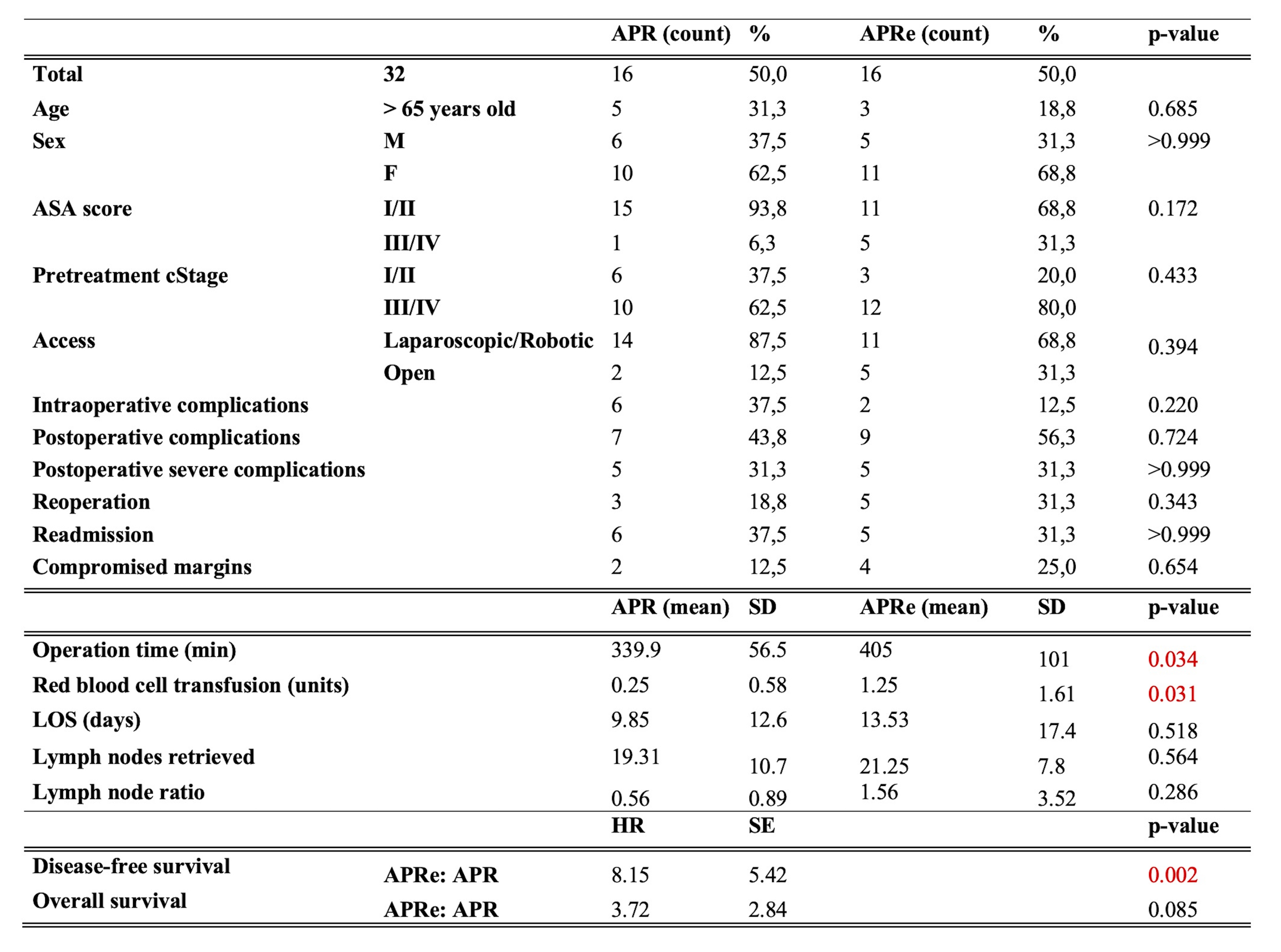
Figure 1. This table compares abdominoperineal resection (APR) with extended abdominoperineal resection (APRe). Red p-values show significant results. M: Male; F: Female; LOS: Length of hospital stay.
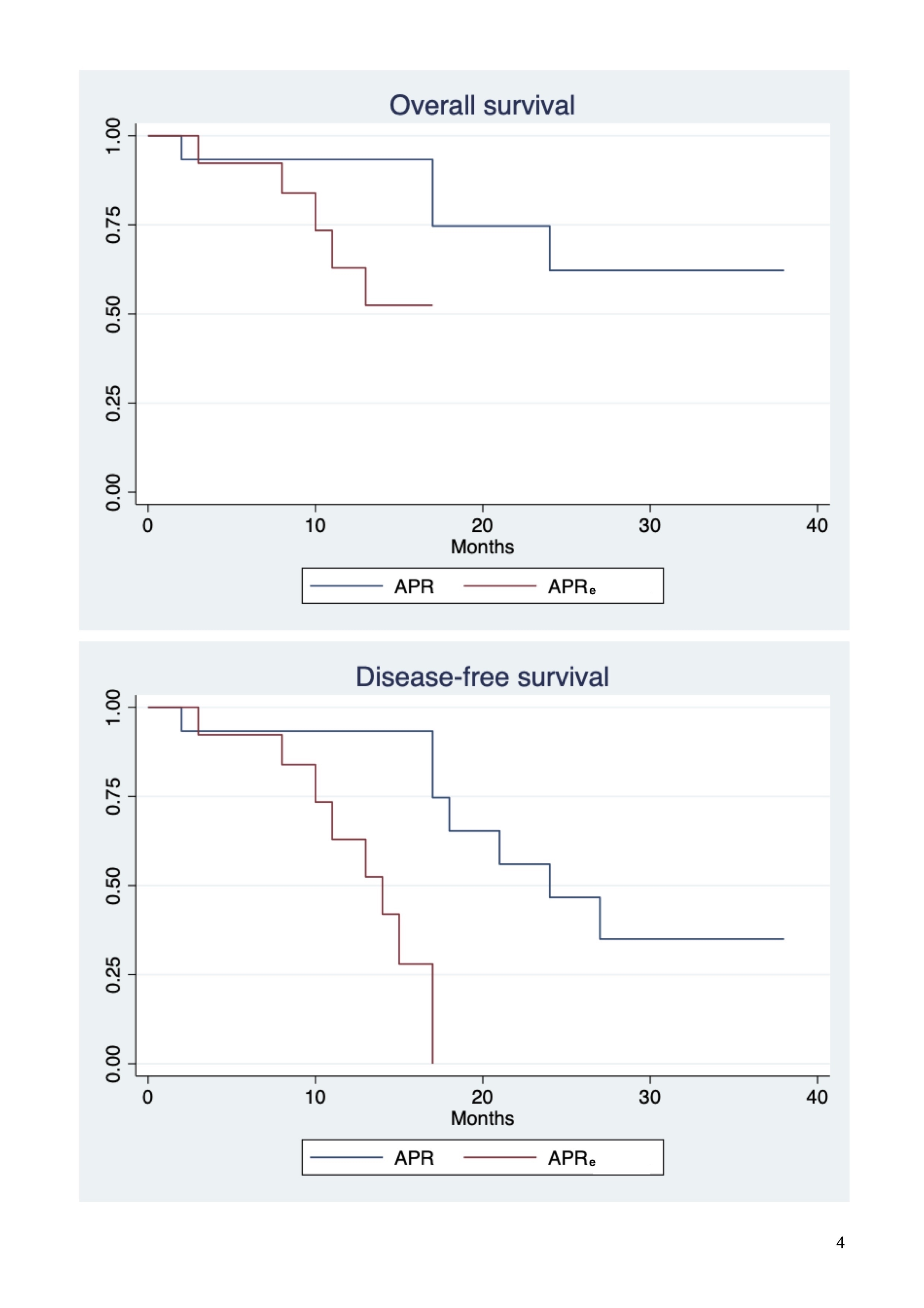
Figure 2. Overall survival and disease-free survival comparison between abdominoperineal resection (APR) with extended abdominoperineal resection (APRe).

