
INTRODUCTION
Mesenteric cystic lymphangiomas are abdominal masses postulated to develop from malformations within the lymphatic vessels, resulting in the failure of drainage of lymphatic fluid. Although they are believed to be congenital anomalies, only 60% present during childhood. This incidence of delayed presentation allows for additional theories on etiology, including prior trauma, surgery, inflammation or radiation that may result in obstruction of lymphatic channels and eventual mass development. Estimated incidence of MCLs has ranged from 1 in 20,000 to 1 in 250,000 people. Presentation in adulthood can be variable, ranging from incidental findings on imaging, to mass effect on intra-abdominal or retroperitoneal organs, to life-threatening obstructions and surgical emergencies. Physical exam may reveal an abdominal mass in up to 60% of patients. Abdominal CT scan is the gold standard for diagnosis; tumors typically appear homogenous, hypodense, with thin partitions and a fatty appearance of chylous liquid. Treatment is excision or marsupialization as there is a risk of life-threatening complications associated with an intraabdominal tethering point. Pathologic evaluation is necessary to rule out underlying malignancy.
CASE REPORT
Our patient is a 31 year-old male with no prior surgical history and only medical history of vague abdominal pain believed to be PUD treated with famotidine and sucralfate who presented to an urgent care for severe abdominal pain over several hours. He had associated bilious emesis and workup showed a leukocytosis of 12, normal lactate, and CT Abdomen and Pelvis with contrast concerning for a possible closed loop obstruction of the small intestine and a 10-15cm cystic mass.
He was taken to the OR for diagnostic laparoscopy, which was converted to laparotomy for a large mesenteric mass. After evisceration of the bowel, the mesenteric cystic mass was seen to be causing volvulus of approximately 35cm of small bowel resulting in ischemia to the bowel. There was chylous injection of the mesentery along the length of this bowel which was resected down to the root of the mesentery and healthy bowel anastomosed in a side-to-side fashion.
After a slow return of bowel function, patient was discharged on post-op day 6 with a relatively uncomplicated hospital course. Final pathology showed benign cystic lymphangioma 8cm in diameter with 2 benign lymph nodes.
DISCUSSION
In a patient with no surgical history, presentation concerning for obstruction, and a cystic or fatty appearing mass on imaging, the diagnosis of Mesenteric Cystic Lymphangioma should be included in the differential. It is worth remembering that these rare tumors are almost universally benign, but pose a risk of mechanical obstruction, perforation, and torsion; therefore, they should be resected.
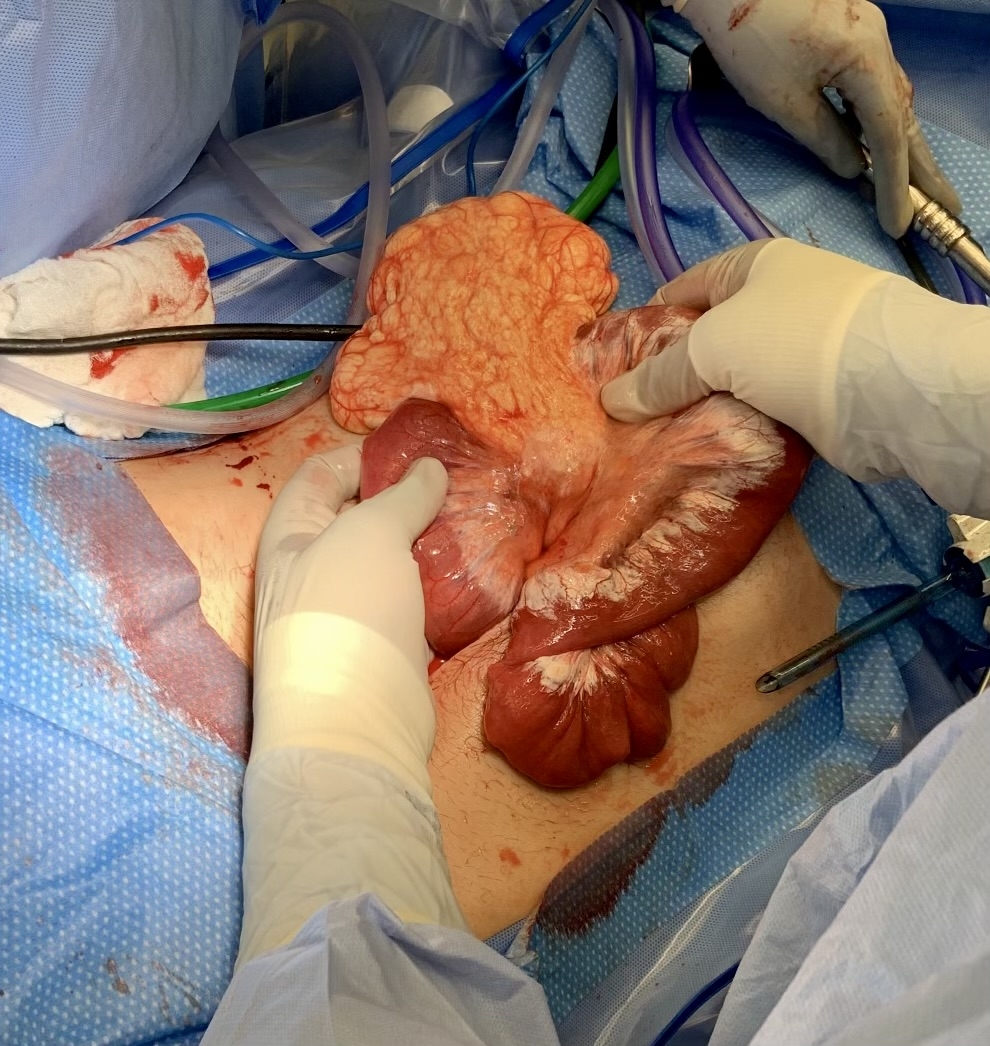
Intra-op view of lesion prior to resection

Specimen after removal

