
Introduction
Endoscopic ultrasound (EUS) guided gastroenterostomy using a lumen apposing metal stent (LAMS) is well described for management of gastric and duodenal obstructions. Rare cases of EUS guided duodenojejunostomy exist in literature.
Case Description
A 79 year old female with a history of proximal jejunal cancer underwent resection with loop gastrojejunal (GJ) anastomosis in 2000. She developed GJ stenosis and stenosis of jejuno-jejunal (JJ) anastomosis and underwent surgical duodenojejunostomy (DJ) with efferent jejunum in 2017. She presented with chronic persistent symptoms of nausea, vomiting and weight loss. CT of abdomen showed a massively dilated duodenum consistent with obstruction of distal duodenum. On push enteroscopy, a stricture of previous GJ anastomosis was seen with a 15cm long benign appearing stenosis of the efferent jejunum able to be traversed with moderate resistance. DJ anastomosis was patent but efferent jejunum stricture was seen 3cm distal to anastomosis, unable to be traversed with scope. Stricture biopsies did not show any recurrent malignancy. After a multidisciplinary discussion with surgical team, given patients frail health, decision was made to perform EUS guided duodeno-jejunostomy. Enteroscopy was performed and a 7Fr nasocystic catheter was placed in the downstream jejunum through GJ anastomosis and across a JJ anastomosis. Efferent Jejunum was distended with saline mixed with contrast and identified on EUS from the third part of duodenum. A cautery enhanced 20mm x 10mm LAMS was successfully placed creating a new duodeno-jejunostomy. Patient was started on a clear liquid diet and subsequently discharged on a regular stent diet. At 3 month followup, patient had gained 13 lbs of weight with complete resolution of nausea and vomiting. No post procedural diarrhea noted.
Discussion
EUS guided gasteroenterostomy using LAMS is predominantly utilized for palliation of malignant obstructions. Performing duodeno-enteric anastomosis poses significant technical challenges with only rare cases described in literature. Duodenum is retroperitoneal and unlike the stomach, can not be mobilized adequately to align adjacent to a jejunum loop. In our case, the surgical anatomy made it challenging to identify appropriate loop of jejunum to perform the anastomosis. To our knowledge, this is the first case of EUS guided duodenojejunostomy described in literature with a complex surgical anatomy and a benign obstruction at two anastomoses.
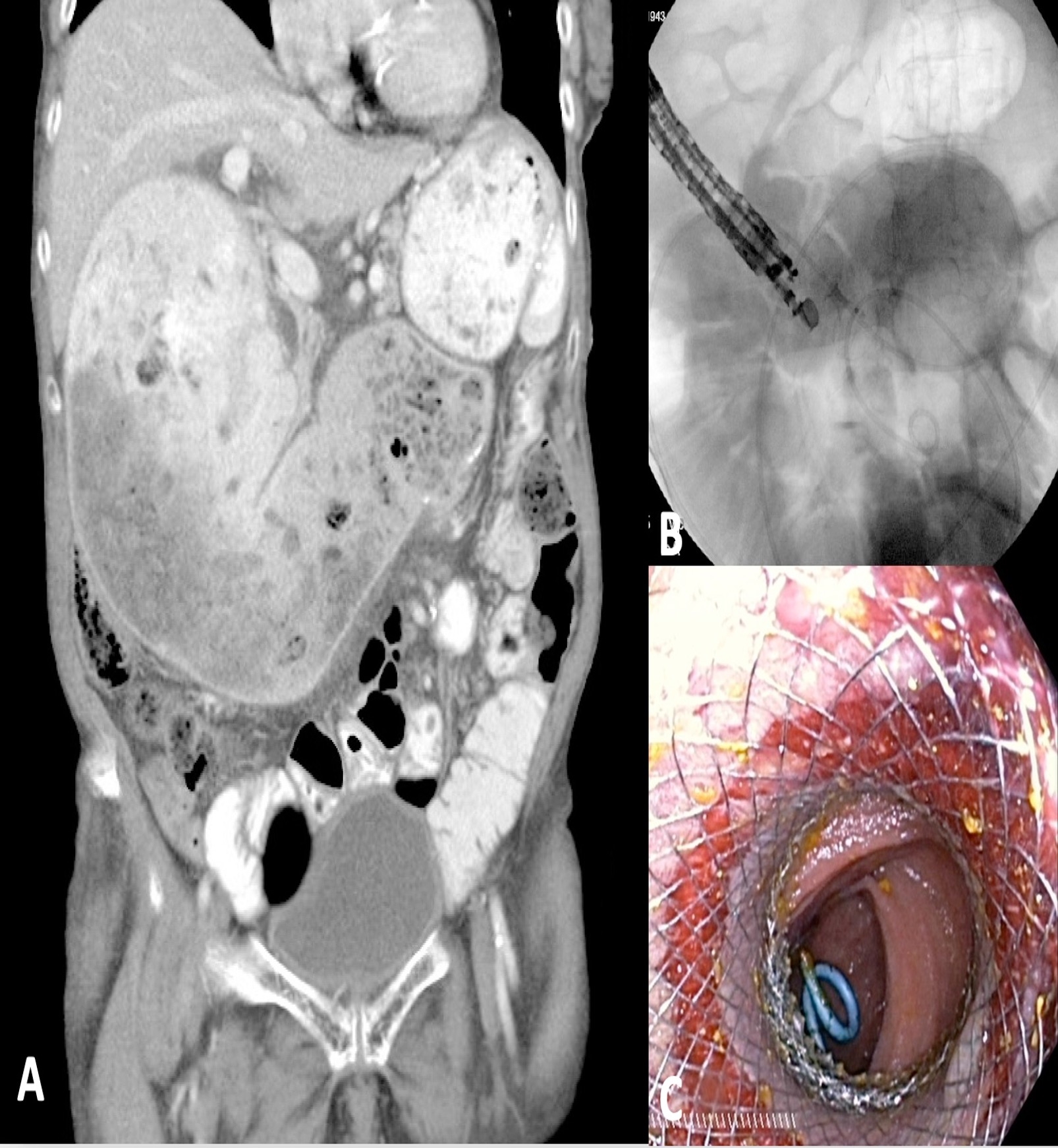
(A)Coronal CT imaging demonstrating massively dilated duodenum with obstruction in distal duodenum, near duodeno-jejunal anastomosis.
(B)Nasocystic catheter with contrast in efferent jejunum and LAMS duodenojejunostomy using linear echoendoscope
(C)Endoscopic view of LAMS with nasocystic catheter and jejunum visualized through the stent

