Background: Meckel’s diverticulum (MD) is the most common congenital anomaly of the gastrointestinal tract, with an incidence up to 3%. The majority of MD patients are asymptomatic. When symptomatic, adults may present with hemorrhage, enteritis, and bowel obstruction, and rarely with enteric fistula. As it is not always identified by computerized tomography (CT), MD is often discovered during emergency surgery. Evidence-based intra-operative decision making is critical for surgical management of symptomatic and incidentally discovered MD.
Objective: To evaluate outcomes of adult patients who were discovered to have MD during surgery.
Methods: We performed a scoping review based on a Medline search using the term “Meckel Diverticulum” over the last two years. We included adult patients who were discovered to have a MD at the time of abdominal exploration; patients with a preoperatively identified MD were excluded. We analyzed patient demographics, CT imaging, presenting symptoms, surgical procedure, and patient outcomes.
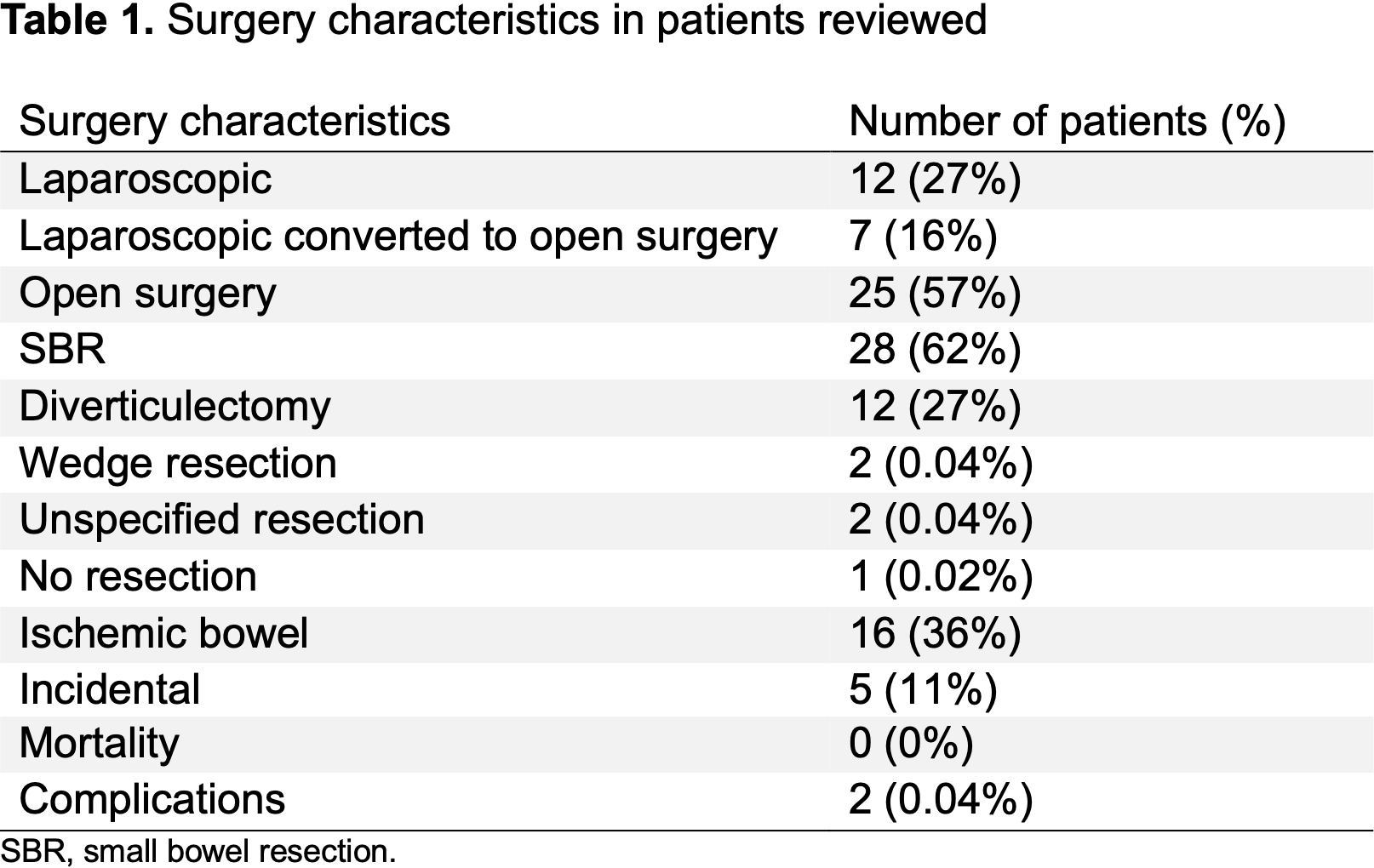
Results: Forty-five patients from 26 countries met the inclusion criteria. The mean age was 42 years; 36% of patients were female; 3 patients were pregnant. Non-diagnostic CT scans were obtained in 76% of patients. Incidental asymptomatic MDs were found in 11% of patients; the MD was resected in 80% of these patients. The MD was symptomatic in 89% of patients. Indication for surgery included bowel obstruction (62%) and gastrointestinal hemorrhage (11%). More than half (51%) of patients had signs of an acute abdomen prior to surgery. Ischemic bowel was identified in 36% of patients. Surgery was performed as an open procedure in 57% of patients; in 16% of patients surgery was converted from laparoscopic to open surgery. Postoperative complications of ileus and intra-abdominal abscess occurred in 4% of patients. No mortality was identified in this scoping review.
Conclusion: MD should be included in the differential diagnosis of abdominal complaints even if not detected by CT imaging. Intra-operative decision-making regarding resection and potential conversion to open can be challenging in these patients. These decisions should be individualized and based on the patient’s clinical status, the surgical findings, and the experience of the surgeon. Simple diverticulectomy and formal small bowel resection with anastomosis can both lead to successful patient outcomes for both symptomatic and incidental MD. Our scoping review highlights the intra-operative decision making and the surgical options when a MD is encountered.