Introduction
Gallstone ileus is an infrequent complication of cholelithiasis and is defined as the mechanical obstruction of the small bowel due to the impaction of a large gallstone usually in the setting of a cholecysto-duodenal fistula. These patients usually require surgery with enterotomy and extraction of stone. We present a rare case of successful endoscopic management of gallstone ileus.
Case Description
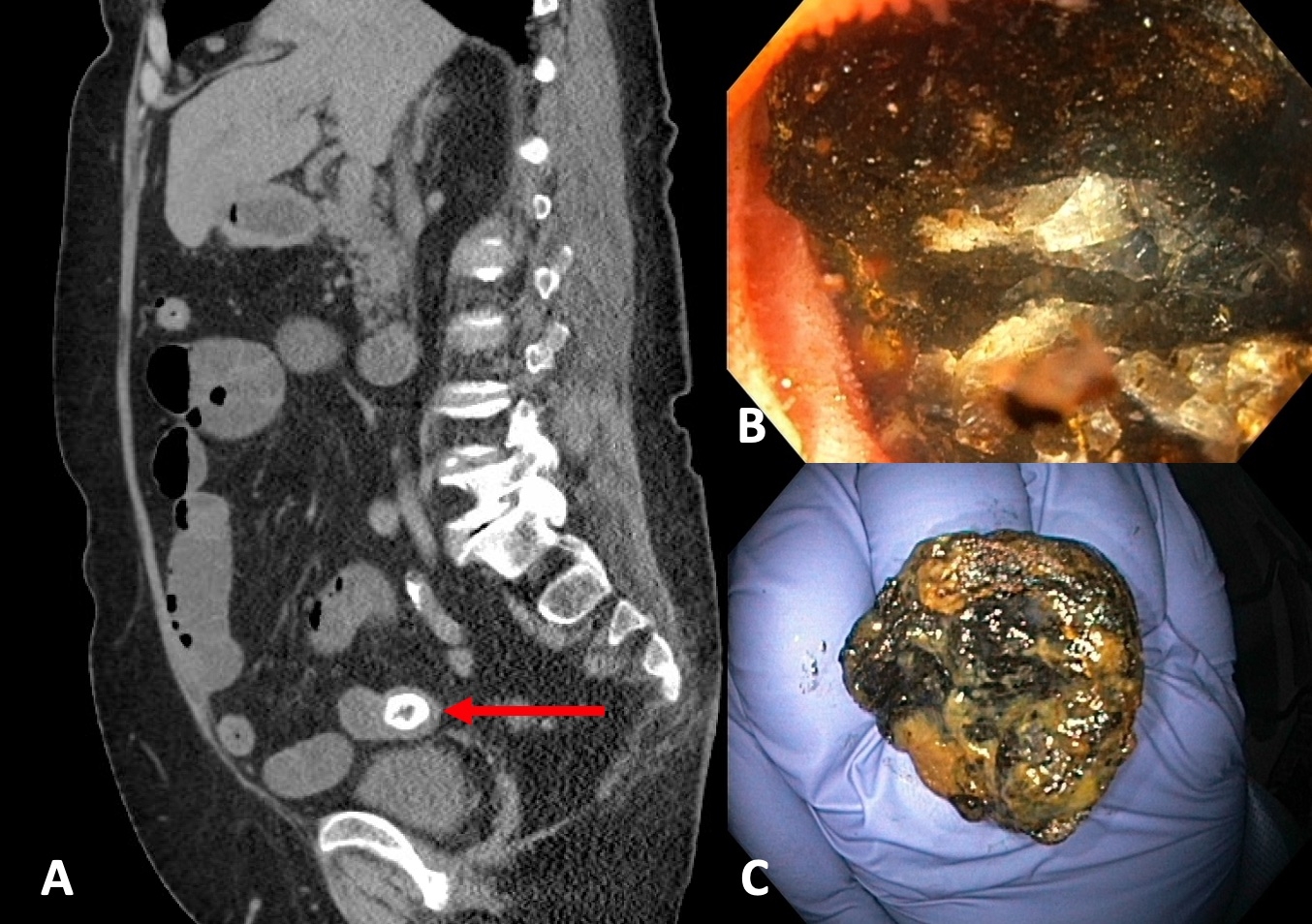
A 78-year-old female presented to the emergency room with 3 days of periumbilical abdominal pain and vomiting. On physical examination, the abdomen was mildly distended without tenderness, guarding, or rigidity. CT scan of abdomen and pelvis showed cholecysto-gastric fistula, cholelithiasis and small bowel obstruction in setting of a large gallstone in the ileum, approximately 15cm upstream of the ileocecal valve (ICV). Multidisciplinary discussion was held with the surgical team and given her frailty, absence of peritonitis, and favorable location of stone, decision was made to attempt endoscopic lithotripsy and stone retrieval. Underwater colonoscopy was performed without a bowel prep and terminal ileum was intubated. Patient was placed in supine position to aid in deep ileal intubation. An obstructing 2.5cm gallstone was visualized 15cm upstream of the ICV. Attempts at dislodging the stone by passing a guidewire upstream and attempting to sweep with an extraction balloon were unsuccessful. Electrohydraulic lithotripsy (EHL) with normal saline immersion was performed and edges of the stone were fragmented to reduce the stone diameter. Once residual stone size was less than 2cm, this was retrieved and removed using a net. Total procedure time was 120 minutes. Post procedure CT with oral contrast showed resolution of obstruction and no residual stone in bowel lumen. The patient’s diet was gradually advanced and patient was discharged home 3 days later with resolution of symptoms.
Discussion
Gallstone ileus is a true mechanical obstruction and is generally considered a surgical emergency. Rare cases of endoscopic lithotripsy to manage these stones have been described in the duodenum and jejunum. To our knowledge, this is the first case of successful endoscopic management of gallstone ileus in a single session with the stone in the ileum upstream of the IC Valve. Underwater colonoscopy without a bowel prep and targeting edges of stone for lithotripsy are helpful for successful stone extraction.