
Background: Preoperative volumetry of the future liver remnant (FLR) is essential to minimize the risk of posthepatectomy liver failure. For volumetry, manual tracing on computed tomography (CT) images is still widely used but may be time-consuming and operator dependent. To overcome these disadvantages, several three-dimensional simulation software programs have been developed; however, their efficacy has not fully been compared to that of manual tracing volumetry.
Study design: Retrospective data were collected on 30 patients who underwent formal right hepatectomy. Three physicians performed liver volumetry on preoperative CT images using manual tracing volumetry and two simulation software programs, SYNAPSE and syngo.via. The standardized FLR (sFLR), defined as the ratio of the calculated left-liver volume to the standardized total liver volume, was calculated using each method of volumetry. The primary endpoint was reproducibility evaluated using Bland-Altman analysis. Secondary outcomes were calculation time and learning curve.
Results: The mean (95% CI) sFLR was 30.1% (27.7–32.5) with manual tracing, 32.0% (29.4–34.6) with SYNAPSE software, and 32.0% (29.5–34.5) with syngo.via software. The mean sFLR was significantly lower for manual volumetry than for SYNAPSE (p = 0.002) or syngo.via (p < 0.001); there was no significant difference in mean sFLR between the two software-based methods (p = 1.000). The sFLR values based on manual tracing volumetry differed significantly between Rater 1 and Rater 2 (p = 0.002), but the sFLR values based on SYNAPSE software (p = 0.587) and syngo.via software (p = 0.154) did not (Figure 1A). The sFLR values based on the different volumetry methods did not differ between Rater 2 and Rater 3 (Figure 1B) or between Rater 3 and Rater 1 (Figure 1C). That is, reproducibility was lower for the manual method than for the software-based methods. The mean (95% CI) calculation time was 42.9 (40.0–45.8) min for manual tracing, 6.4 (5.4–7.5) min for SYNAPSE software, and 10.8 (9.7–11.8) min for syngo.via software (p < 0.001) (Figure 2). For the two physicians unfamiliar with the software, no obvious learning curve was observed for using SYNAPSE, whereas learning curves were observed for using syngo.via.
Conclusions: Liver volumetry was more reproducible and faster with three-dimensional simulation software, especially SYNAPSE software, than with the conventional manual tracing method. Software can help even inexperienced physicians learn quickly how to perform liver volumetry.
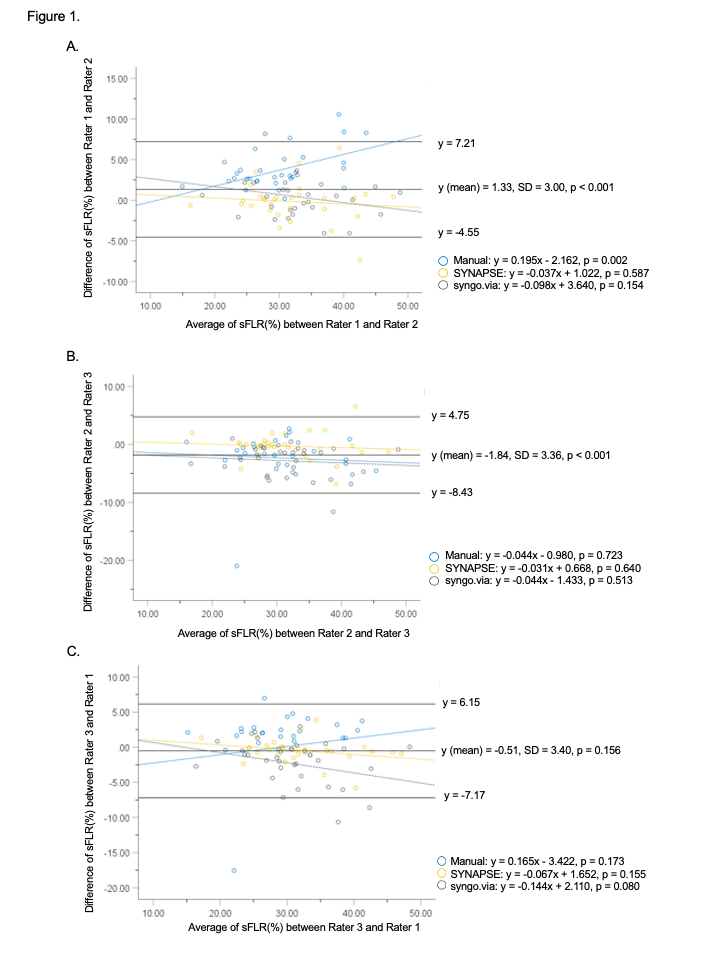
Comparison of standardized future liver remnant between three methods and between three physicians. The mean values and 95% CIs are indicated with circles and error bars, respectively.
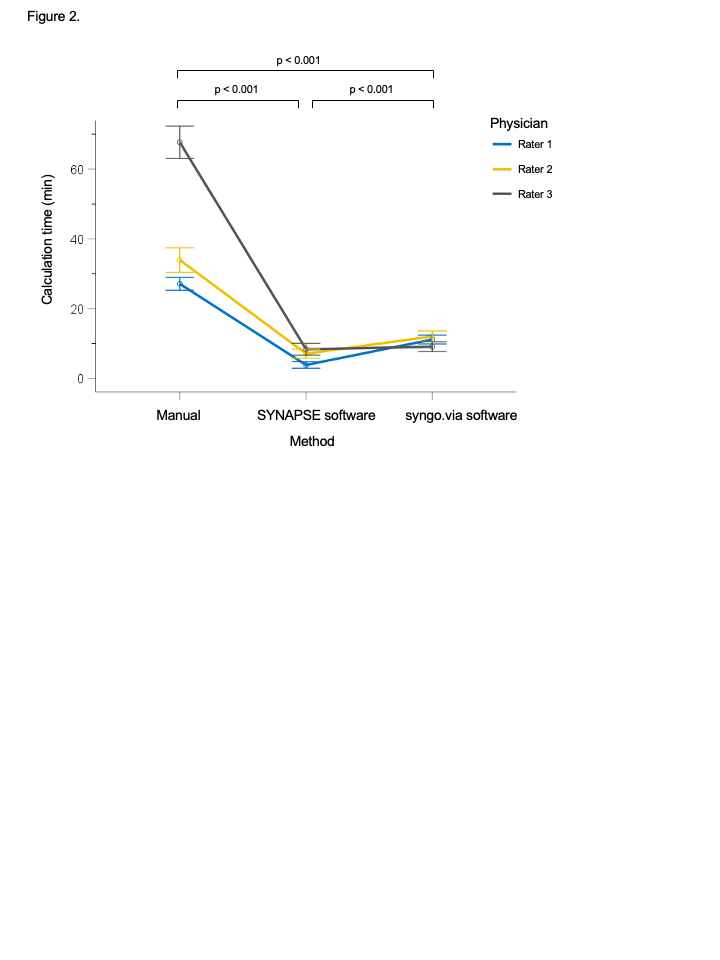
Comparison of calculation time between the three methods and between the three physicians. The mean values and 95% CIs are indicated with circles and error bars, respectively.

