
Background:
Common bile duct (CBD) stones has a prevalence of 10-20% in patients with gallstones and are especially common in the North Indian population with multiple, large and impacted stones. These are usually mixed type of stones and offer significant challenges for extraction by Endoscopic Retrograde Cholangio-Pancreaticography (ERCP) and endoscopic sphincterotomy. Amongst the various options available, laparoscopic common bile duct exploration (LCBDE) is the favoured approach in dealing with multiple stones in a dilated bile duct. We report our experience of LCBDE spanning over a decade with long term follow-up.
Methods:
Between 2010 and 2023, 183 cases with documented CBD stones in dilated ducts were treated laparoscopically using the trans-choledochal approach. All basic investigations were performed and pre-operative MRCP was done in all cases for visualization of biliary anatomy and stone load. One extra port was added to the conventional 4 ports of laparoscopic cholecystectomy (Figure 1). Supra-duodenal choledochotomy was performed using a needle tip hook using monopolar energy. Intraoperative choledochoscopy was performed in all patients using 8/10 Fr rigid ureteroscope to visualize and remove the CBDS under vision and to check for completion of removal at the end of the procedure. The calculi were extracted using a 10mm right-angled dissector in combination with Dormia basket/balloon trawling/holmium laser lithotripsy under choledochoscopic vision, where required. Stone clearance was confirmed with choledochoscopy of the upper biliary tract from the umbilical port where right and left hepatic ducts and the segmental ducts were clearly identified. Stone clearance of the distal CBD was confirmed by choledochoscopy from the epigastric or additional 5 mm subcostal port with visualisation of ampulla and entry of the ureteroscope into the duodenum (Figure 2). A 7 Fr 10 cm long endobiliary stent was placed in all cases and the choledochotomy was closed using continuous 3-0 polygalactin suture.
Results:
There were 28 males and 155 females with age ranging from 18 to 70 years. The mean size of the CBD on ultrasound was 12.4 +/- 3.2 mm and on MRCP 13.8 +/- 4.1 mm. The number of stones extracted varied from 1 to 70 and the size of the extracted stones from 5 to 30 mm. The average duration of surgery was 148.0 +/- 20.5 min (range 90 - 228 min) and the mean intraoperative blood loss was 133.5 +/- 57.6 ml. There were 3 conversions to open procedures (1.63%) and 15 patients (8.19 %) had nonfatal postoperative complications. There were no mortality. Two patients had retained stones (1.09 %) and one developed recurrent stone (0.54%). Mean post-operative hospital stay was 2.4 days.
Conclusions:
LCBDE is a safe and feasible procedure with near 100% complete clearance of the CBD using rigid choledochoscopy in dilated common bile ducts and large stone load.
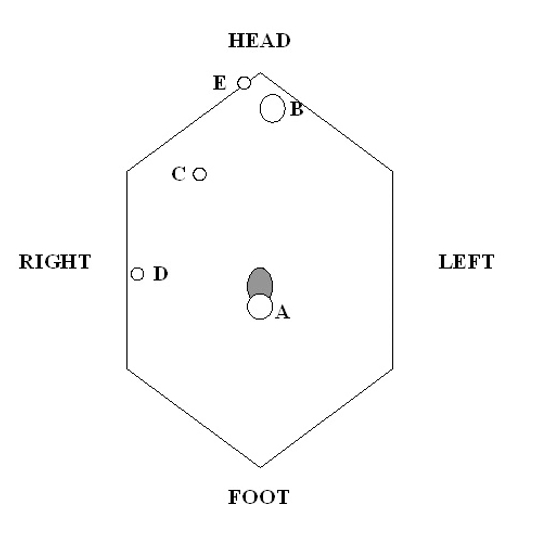
Fig 1 : Port Positions
Figure 2. 1) Retrieval of stone using Dormia basket; 2) Choledochoscopy- right and left hepatic ducts; 3) Choledochoscopy- ampulla opening into duodenum; 4) Choledochoscopy- right segmental ducts; 5) MRCP- multiple CBD stones; 6) Multiple CBD stones retrieved.

