Introduction: Medicare determination of reimbursement rates for medical services plays a pivotal role in shaping the financial framework of healthcare delivery in the United States. Medicare reimbursement rates set a benchmark for commercial insurance companies. Previous studies have outlined a decline in Medicare reimbursements across various surgical specialties including colorectal surgery, but this has yet to be explored in upper gastrointestinal (UGI) cancer surgery. This study evaluates the trend in reimbursement rates for UGI cancer operations.
Methods: The Physician Fee Schedule Look-Up Tool from the Centers for Medicare & Medicare Services (CMS) was queried for Current Procedural Terminology (CPT) codes of 20 common UGI operations employed for cancer, spanning from 2003 to 2023. The total annual Medicare reimbursement for each CPT was determined by multiplying the procedure specific relative value unit (RVU) with the overall conversion factor (CF). The raw yearly percent change in Medicare reimbursement from 2003 to 2023 was calculated for each CPT. To account for inflation, percent change was compared to the change in the general consumer price index (CPI) for the same time. The adjusted compound annual growth rate (CAGR) for each CPT was calculated using inflation-adjusted data. A p<0.05 was considered statistically significant. Subgroup analysis based on operation type (gastric, small bowel, palliative enteral access for decompression/feeding, and esophageal) was performed.
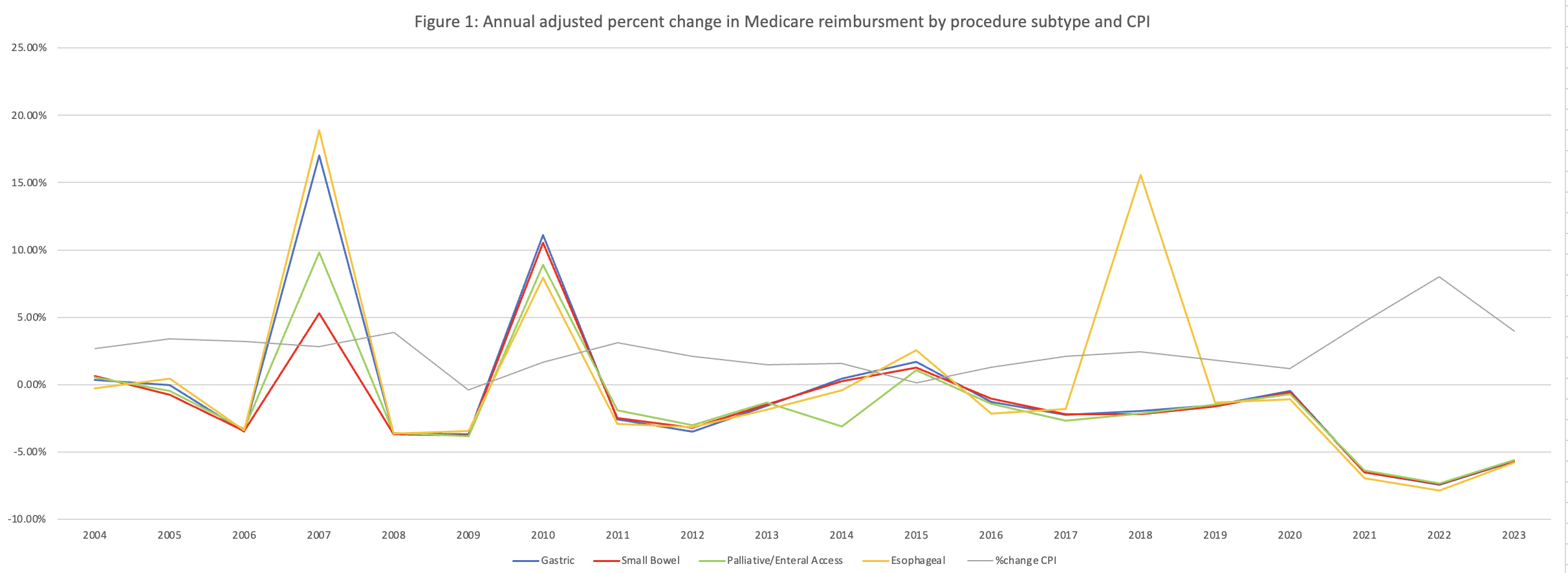
Results: From 2003 to 2023, the median unadjusted percent change for the 20 UGI operations quired was +31.27% (IQR 22.19% to 48.03%). During the same time, the CPI increased by 69.15% (p<0.001). After adjusting for inflation using the yearly CPI % change, the median percent change for the 20 UGI operations was -20.63% (IQR -26.22% to -8.43%). The adjusted average yearly CAGR was -1.15% (standard deviation SD 0.81%). Over the study period, only two queried procedures (distal gastrectomy with gastrojejunostomy and partial esophagectomy with colonic interposition or small bowel reconstruction) saw an increase in Medicare reimbursement of +0.14% and +14.39%, respectively. All analyzed subgroups of operation types saw an average decrease in Medicare reimbursements with gastric at -16.19% (SD 10.6%), small bowel at -25.7% (SD 4.6%) palliative at -25.12% (SD 15.55%), and esophageal at -7.64% (SD 15.06%) (Figure 1).
Conclusion: Inflation-adjusted Medicare reimbursement rates for common UGI cancer operations have declined in the past twenty years. It is important for surgeons, policy makers, and hospital administrators to recognize this trend and consider the impact it may have on access to high-quality surgical care.