Back to 2024 Abstracts
COMPREHENSIVE REPORT CARD ANALYSIS OF ACHALASIA AFTER MYOTOMY SHOWS SIMILAR OUTCOMES ACROSS SUBTYPES
Archana Jeeji
*1, Ealaf Shemmeri
2, Peter T. White
1, Adam J. Bograd
1, Alexander S. Farivar
1, Brian E. Louie
11Thoracic Surgery, Swedish Medical Center, Seattle, WA; 2Brigham and Women's Hospital, Boston, MA
Background
Achalasia is classified into three subtypes with variable responses to the known treatment options. Type II responds best to any treatment whereas Type I has less improvement. Both have better treatment response compared to Type III. Recent clinical guidelines recommend peroral endoscopic myotomy (POEM) for Type III due to its ability to achieve a tailored, longer, proximal myotomy. Studies supporting these recommendations define treatment success by a single outcome: an Eckhart score ≤ 3. We hypothesize that comparing key outcomes using a comprehensive report card across the three achalasia subtypes will demonstrate similar results regardless of subtype.
Methods
We performed a retrospective chart review of patients with primary achalasia undergoing POEM or Heller myotomy with or without fundoplication from January 2005 to May 2023. Outcomes were assessed using a comprehensive report card including 1) patient reported outcomes using the Eckardt score and GERD-HRQL; 2) objective measures of success with timed barium swallow (TBS) clearance by 5 min, integrated relaxation pressure (IRP) <15mm Hg, presence of esophagitis and pH testing; and, 3) the need for re-intervention. The most recent encounter was assessed.
Results
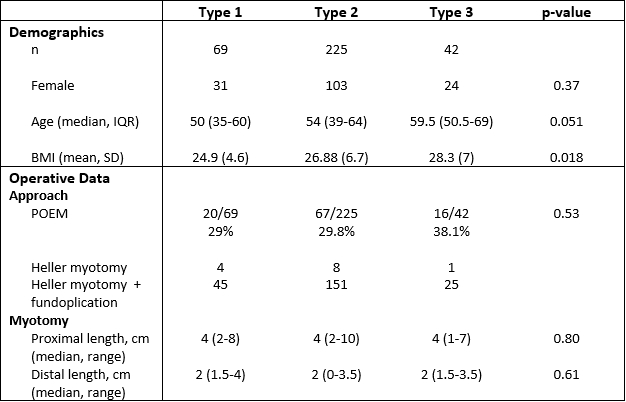
There were 336 patients including Type 1 (69), Type II (225) and Type III (42) patients. Age and gender were similar. Patients with Type I achalasia had a lower BMI at presentation. There was no significant difference in choice of operation or myotomy lengths amongst the subtypes.
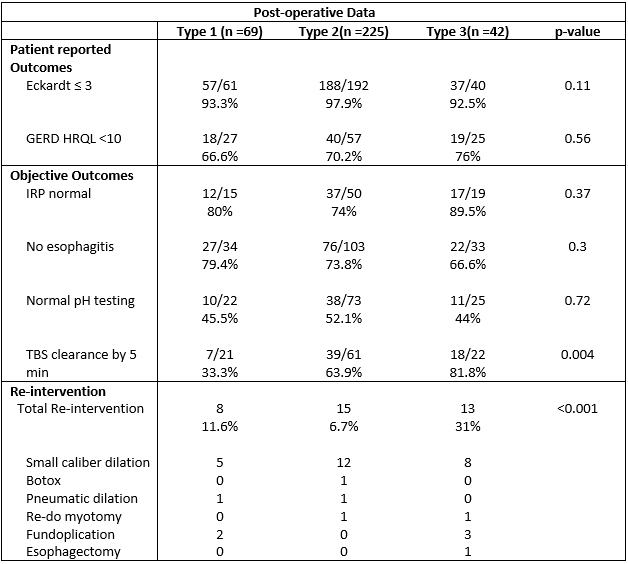
After myotomy, all three subtypes reported similar symptomatic treatment responses as defined by an Eckardt score ≤3. Type I had higher rates of symptomatic GERD defined by a GERD HRQL ≥ 10.
The median IRP was normalized in all groups with Type II having the highest rate. Type I patients had delayed post-operative clearance on TBS whereas Type III cleared though not different.
Types I and III showed higher rates of reflux on pH testing when compared to Type II. Type III developed more esophagitis post-myotomy.
Re-intervention occurred in 13/42 (31%) of Type III patients versus 8/69 (11.6%) for Type 1 and 15/225 (6.7%) for Type II (p<0.001).
Of those with Type III needing surgical re-intervention, 1 underwent esophagectomy for end-stage achalasia, 2 had Toupet fundoplication for reflux and 1 underwent POEM after Heller/Dor. Both patients with Type I achalasia needing surgical re-intervention underwent a Toupet fundoplication after POEM for reflux. One patient with Type II underwent Heller/Dor after POEM for persistent dysphagia.
Conclusion
All subtypes have excellent post-myotomy Eckardt scores. Type III showed better emptying with higher rates of normal IRP and clearance on TBS but had more reflux-related morbidity and required more re-interventions compared to its counterparts. Many of the re-interventions were related to reflux, not treatment failure.
Back to 2024 Abstracts


