Back to 2024 Abstracts
MESENTERIC LENGTHENING TECHNIQUES FOR ILEOANAL POUCH CONSTRUCTION: WHAT TO DO WHEN THE POUCH WON'T REACH
Megan Obi
*, John Mcmichael, Jie Dai, Emre Gorgun, Tracy L. Hull, Arielle E. Kanters, Hermann Kessler, Olga Lavryk, Jeremy M. Lipman, Michael Valente, Scott Steele, Stefan D. Holubar
General Surgery, Cleveland Clinic, Cleveland, OH
During ileal pouch-anal anastomosis (IPAA), difficulty in reaching the pelvic floor and excess mesenteric tension on the pouch are technical challenges that surgeons must overcome, and excess tension may be associated with increased anastomotic leak rates. We aimed to describe practice variations in utilization of lengthening maneuvers and outcomes in mesenteric lengthening during IPAA. We hypothesized patients who required lengthening maneuvers, compared to those who did not, had similar pouch leak rates.
MethodsA retrospective single-center review of a sample of IPAA patients from a prospectively maintained pouch registry was conducted for all adult patients who underwent IPAA creation between 1994 and 2021. A natural language processing (NLP) search was performed for lengthening keywords and phrases in operative reports, all (100%) of which were manually reviewed.
ResultsOf the 517 potential cases of mesenteric lengthening identified via NLP, we confirmed 195 (37.7%) cases underwent at least one lengthening maneuver. A total of 80 (41.0%) were laparoscopic or robotic, and 12 (6.2%) were converted from laparoscopic to open, of which 2 (16.7%) were converted after lengthening was attempted. The most utilized maneuvers in both minimally invasive and open cases were complete mobilization of the superior mesenteric artery (SMA) to the 3
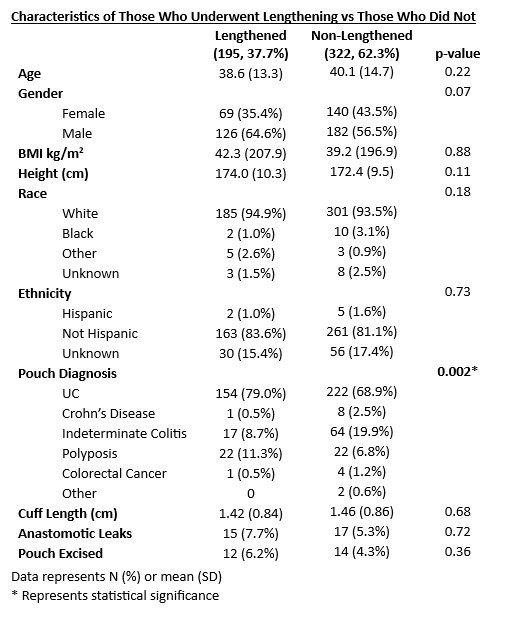
rd portion of the duodenum in 136 (69.7%) cases and scoring of the small bowel mesentery in a stepladder fashion in 106 (54.4%). Other maneuvers included high ligation of the ileocolic (66, 33.8%), excision of the bowstring of avascular mesentery lateral to the SMA (48, 24.6%), duodenal kocherization (25, 12.8%), ligation of SMA branches (6, 3.1%), and ligament of Treitz takedown (1, 0.5%). The median number of maneuvers utilized per case was 2. Lengthening maneuvers were most utilized after anorectal transection (137, 70.3%) and colorectal specimen removal (133, 68.2%), but before pouch construction (161, 82.6%). An S-pouch was required to reach the anus in 20 cases (10.3%). There was no significant difference in mean age (38.6 vs. 40.1 yrs, p=0.22), BMI (42.3 vs. 39.2 kg/m
2, p=0.88), height (174.0 vs. 172.4 cm; p=0.11), pouch leak rate (7.7% vs. 5.3%; p=0.72), and pouch excision rate (6.2% vs. 4.3%, p=0.36) between patients who underwent lengthening maneuvers and those who did not.
ConclusionMesenteric lengthening maneuvers are critical to achieving pouch reach, but despite these maneuvers, an S-pouch was required in 10%. Patients who required lengthening were observed to have a similar leak rate compared to those who did not. Further research into predictors of difficulty in reach may help surgeons anticipate when mesenteric lengthening maneuvers may be needed.
Back to 2024 Abstracts


