Back to 2024 Abstracts
IMPACT OF HOSPITAL FLAGSHIP SYSTEM AFFILIATION ON SURGICAL OUTCOMES FOLLOWING COMPLEX CANCER SURGERY
Muhammad Musaab Munir
*, Selamawit Woldesenbet, Muhammad Muntazir M. Khan, Susan Tsai, Timothy M. Pawlik
Surgery, The Ohio State Wexner Medical Center, Columbus, OH
Introduction: Affiliation with a major regional hospital system is often promoted to patients as an opportunity to benefit locally from the same standard of care experienced at the flagship hospital. We sought to evaluate variations in patient outcomes following complex cancer surgery at flagship hospitals versus flagship affiliates.
Methods: Medicare 100% Standard Analytic Files were used to identify patients with lung, esophageal, gastric, hepatopancreaticobiliary, or colorectal cancer who underwent surgical resection between 2018 and 2021. A “flagship hospital�? within each region was defined as the major teaching hospital with the highest patient volume that was also part of a hospital system; its system was categorized as a “flagship system.�? Propensity score matching (PSM) was performed to create a 1:1 matched cohort that was well-balanced with respect to covariates. Multivariable regression was used to assess the association between flagship hospitals, affiliates and outcomes.
Results: Among 110,670 patients, a cohort of 55,335 patients who received care within a flagship hospital system (median age, 73 years [IQR, 69-79 years]; n=26,061 (47.1%) male) was matched with 55,335 patients who did not (median age, 73 years [IQR, 69-79 years); n=25,954 (46.9%) male) across 35 regions. Among flagship systems, 7,531 (13.6%) patients underwent care at flagship hospitals. Compared with non-flagship system hospitals, flagship hospitals were more likely to have more beds (mean ± SD: 1090 ± 572 vs. 428 ± 364), be teaching hospitals (39.1% vs. 21.8%), and have higher nurse-bed ratios (3.2 ± 0.9 vs. 2.2 ± 2.9) (all p<0.001). In contrast, flagship affiliate hospitals had equivalent number of beds (384 ± 260 vs. 402 ± 339), teaching hospital status (26.2% vs. 26.5%), and nurse-bed ratios (2.3 ± 1.5 vs. 2.1 ± 2.3) to non-flagship system hospitals (all p>0.05). Patients treated at flagship system hospitals had lower 30-day mortality versus individuals treated at non-flagship affiliated hospitals (4.2% vs 4.9%; OR 0.83, 95%CI 0.79-0.88; p<0.001). Similarly, patients treated at either the main flagship hospital (2.8% vs 4.2%; OR 0.59, 95%CI 0.49-0.72, p<0.001) or at a flagship affiliate hospital (4.4% vs 5.0%; OR 0.86, 95%CI 0.81-0.92) had lower 30-day mortality versus patients receiving care at a non-flagship system hospital (both p<0.001). Importantly, among patients treated within a flagship system, patients treated at the main flagship hospital had a more pronounced reduction in 30-day mortality following a surgical procedure for cancer (main flagship vs. affiliate hospital, OR 0.73, 95%CI 0.62-0.84, p<0.001).
Conclusions: Affiliation with a flagship system was associated with lower risk of 30-day mortality following complex surgery for cancer. However, treatment at the main flagship hospital provided the most benefit relative to odds of peri-operative mortality.
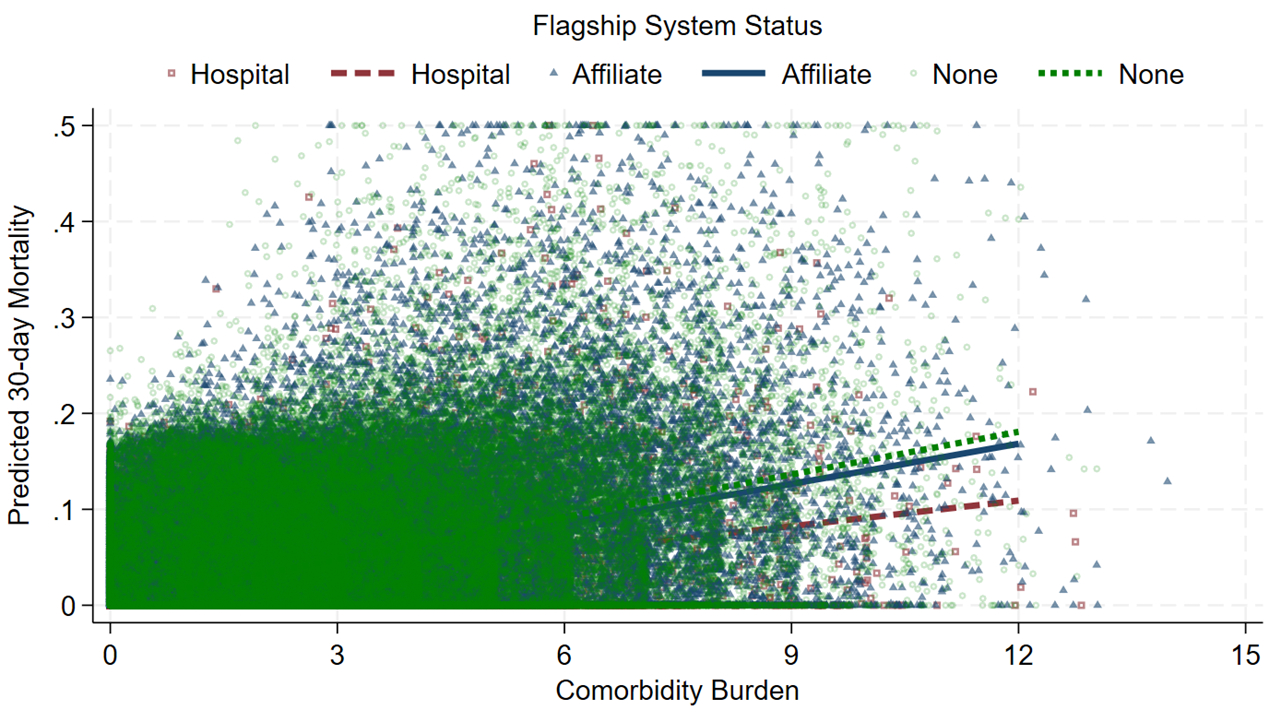
Association between risk of 30-day mortality, and comorbidity burden relative to flagship system status.
Back to 2024 Abstracts


