Back to 2024 Abstracts
TYPE I CHOLEDOCHAL CYSTS IN ADULTS: NATURAL HISTORY AND IMPLICATIONS FOR MANAGEMENT
Alexandra M. Roch
*1, Sonal Walia
1, Mohammed Saad
1, Katelyn Flick
1, Thomas K. Maatman
1, James Butler
1, Trang Nguyen
1, Eugene P. Ceppa
1, Nicholas J. Zyromski
1, Attila Nakeeb
2, Omer Saeed
1, Michael G. House
11Indiana University School of Medicine, Indianapolis, IN; 2Lahey Hospital and Medical Center, Burlington, MA
Background: Historical pediatric data recommend surgical resection for type I choledochal cysts due to the risk of malignant progression over time up to 30%. With the wide use of high-resolution cross-sectional imaging, isolated dilation of the extrahepatic biliary tree has become more frequently recognized. The pediatric management strategy for choledochal cysts has been extrapolated to adults without any specific long-term data. The purpose of this study was to characterize the natural history of choledochal cysts in adults.
Methods: We updated our previously published institutional series. From 1990 to 2023, all adult patients with a radiographic diagnosis of Todani type I choledochal cyst were identified from endoscopic, radiologic, and surgical databases at a single academic institution. All patient demographics, clinical data, imaging studies, pathology, and management outcomes were reviewed.
Results: 100 patients with a median age of 41 years [range 15-78 yrs] and male/female ratio of 0.3 were identified. Eighty-nine patients underwent an operation due to clinical symptoms with or without abnormal serologic liver function tests. Indications for operation included biliary colic symptoms (62%), pancreatitis (16%), and cholangitis (11%). Radiographic median duct size was 22mm [range 9-100]. 73% of patients underwent ERCP as part of work-up. An anomalous pancreaticobiliary ductal junction (APBDJ) was identified in 83% (compared to 30% in biliary dilation from other etiology, p<0.001). Median time from diagnosis to resection was 7 months [range 0.1 – 9 yrs]. The rate of cholangiocarcinoma was 6% during a median follow-up of 8 years [range 0.5-64yrs]. 5/6 (83%) malignant cysts were initially diagnosed during childhood but not resected or only bypassed. Overall morbidity after choledochal cyst resection was 50%, with Clavien-Dindo III-IV complications occurring in 40% patients. Clinically relevant bile leak rate was 15%, with no predictive features on multivariable analysis. Bilioenteric anastomotic stricture and symptomatic retained cyst in the intrapancreatic portion of the bile duct requiring reoperation occurred in 22% and 5% of patients, respectively.
Conclusion: This largest western series of type I choledochal cysts in adults confirms a risk of malignant transformation lower than previously described, occurring mostly in cysts diagnosed during childhood but not resected at that time. When diagnosed at an older age, the lower risk for cholangiocarcinoma should be weighed against the high risk of short- and long-term biliary complications associated with resection including biliary fistula, stricture and recurrent pancreatitis from retained cyst within the intrapancreatic bile duct.
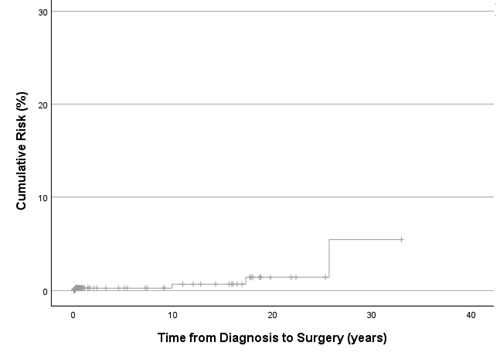
Cumulative risk of malignancy in patients with Todani type I choledochal cysts over time
Back to 2024 Abstracts


