Back to 2024 Abstracts
ENDOLUMINAL VACUUM THERAPY FOR POUCH LEAKS AFTER ILEAL POUCH-ANAL ANASTOMOSIS
Ali Alipouriani
*1, Olga Lavryk
1, Jeremy M. Lipman
1, Tracy L. Hull
1, David Liska
1, Scott Steele
1, Stefan D. Holubar
21Colorectal Surgery, Cleveland Clinic, Cleveland, OH; 2Cleveland Clinic, Cleveland, OH
Background: Anastomotic leakage is a dreaded complication after ileal pouch-anal anastomosis (IPAA) that occurs in 5-10% of cases. Endoluminal vacuum (EndoVac) therapy has emerged as a minimally invasive option that promotes healing by applying negative pressure to the associated abscess cavity through the anastomotic defect but is typically applied only to early IPAA leaks. We hypothesized that EndoVac for early compared with late leaks would be associated with a higher pouch survival rate.
Methods: We retrospectively reviewed the medical records of consecutive patients who developed a pouch anastomotic leak after IPAA and were treated with EndoVac therapy at our institution between 2005-2023. Patients were stratified into early (30 days) and late (>30 days) leaks. Anastomotic healing was defined as complete closure of the leak site, as evidenced by resolution of symptoms, normal endoscopic and radiographic evaluation, and no further drainage from the presacral space or abdominal wall. Pouch failure was defined as a permanent ileostomy or pouch excision. Figures represent frequency (proportion) or median (range). The probability of pouch survival over time was estimated using the Kaplan-Meier method.
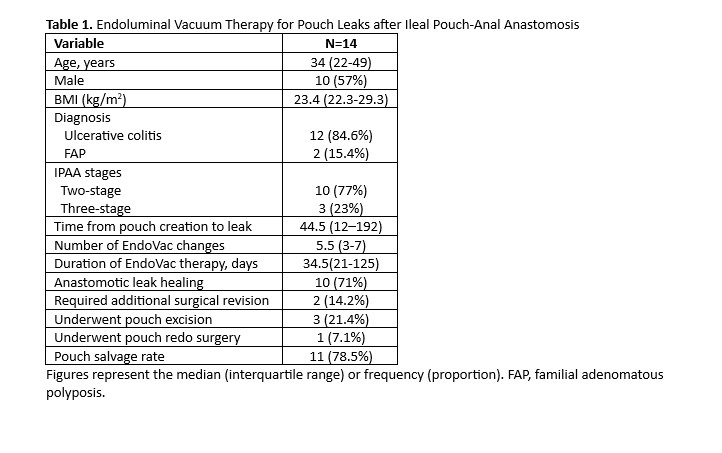
Results: A total of 14 IPAA patients who underwent EndoVac therapy for anastomotic leaks were identified. The median age was 34 years, 57% were male, and the median body mass index was 23.46 kg/m
2. Diagnoses included ulcerative colitis (n=12) and familial adenomatous polyposis (FAP, n=2). The median time from pouch construction to leak was 44.5 (12–192) days; of these, 6 (43%) were early and 8 (57%) were late. All (100%) leaks were at the anal anastomosis site, and all (100%) patients were diverted at the time of EndoVac therapy: 10 (71%) were still diverted and 4 (29%) were re-diverted. Patients underwent a median of 5.5 EndoVac changes (IQR:3-7) over a median duration of 34.5 (21-125) days from initiation of treatment to cessation of therapy. At the end of EndoVac therapy, healing of the leak was observed in 10 (71%) patients, 2 of whom required a minor handsewn revision of the anastomosis; the remaining 4 did not heal and underwent transabdominal surgery: 3 pouch excision and 1 redo pouch surgery. The rates of anastomotic healing (66.7% vs. 75%, p=1.0) and pouch survival (83.3% vs. 75%, p=1.0) were not significantly different between the early and late leak groups. Among those who healed after EndoVac therapy, a total of 8/10 (77.8%) had their diverting loop ileostomy reversed. The overall pouch salvage rate was 78.5%.
Conclusions: EndoVac therapy is effective for postoperative pouch leaks and achieves a high rate of pouch salvage in both early and late leaks.
Back to 2024 Abstracts


