Back to 2024 Abstracts
SHORT- AND LONG-TERM PATENCY AFTER MESOPORTAL VENOUS RECONSTRUCTION DURING PANCREATECTOMY
Brittany C. Fields
*, Antony Haddad, Laura R. Prakash, Jessica E. Maxwell, Michael P. Kim, Naruhiko Ikoma, Rebecca A. Snyder, Jeffrey E. Lee, Matthew Katz, Ching-Wei D. Tzeng
The University of Texas MD Anderson Cancer Center Division of Surgery, Houston, TX
IntroductionEarly loss of mesoportal venous patency after reconstruction during pancreatectomy is often due to technical factors, whereas delayed loss is often associated with disease recurrence. Although there are various techniques for reconstruction, the patency rates of each technique have not been well-defined. This study aimed to assess 1-month and 1-year patency for each technique.
MethodsThis single-institution, retrospective cohort study included patients who had curative-intent pancreatectomy for pancreatic adenocarcinoma from 02/1998-12/2022. Tumor anatomy was assigned based on intraoperative tumor-vein relationship: adherent to or inseparable from the vessel surface (“adherent�?) or concerning for gross invasion (“involvement�?). When available, post-operative imaging was reviewed for short- (1 month) and long-term (1 year) patency of the mesoportal veins.
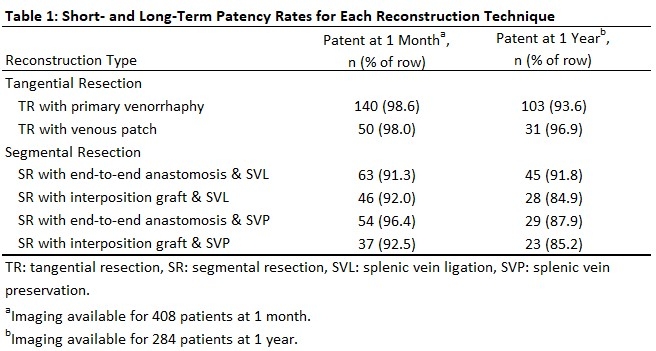
ResultsOf 442 patients, 88.7% (392) underwent pancreatoduodenectomy, 7.0% (31) distal pancreatectomy (DP), and 4.3% (19) total pancreatectomy. Reconstructions included tangential resection (TR) with primary repair (34.4%, 152/442) or vein patch (12.7%, 56/442); segmental resection (SR) with primary anastomosis and splenic vein ligation ([SVL] 16.5%, 73/442) or without SVL (13.8%, 61/442); and SR with interposition graft with SVL (12.9%, 57/442) or without SVL (9.7%, 43/442).
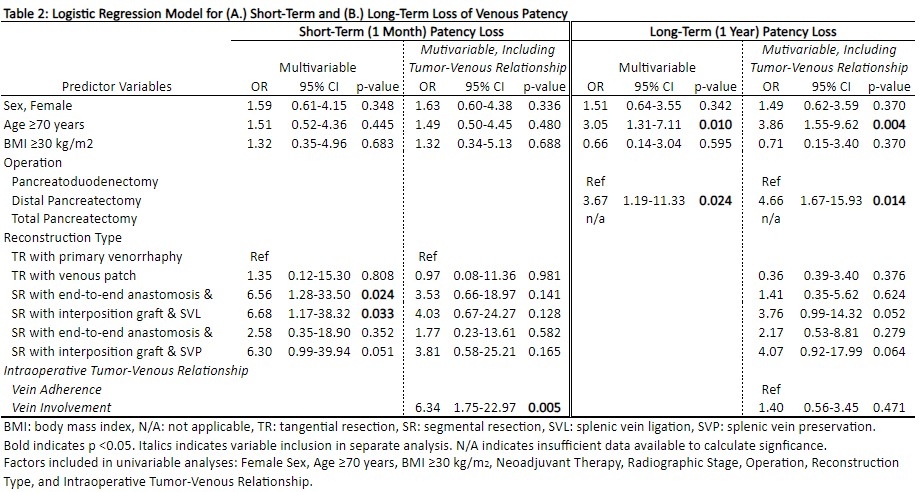
One-month patency was 95.6% (390/408), highest in TR (98.4%, 190/193) and SR without SVL (94.8%, 91/96; p=0.05; Table 1). One-year patency was 91.2% (259/284), highest in TR (94.4%, 134/142) and SR with primary anastomoses (90.2%, 74/82). By multivariable analysis, no technique was strongly associated with maintained patency. Without considering intraoperative tumor-vein relationship, SR with SVL was associated with loss of patency at 1 month (Table 2A), while age ≥70 years, operation, and technique were independently associated with loss of patency at 1 year (Table 2B). When controlling for the tumor-vein relationship, reconstruction technique was no longer associated with patency loss. Vein involvement (OR 8.45, p=0.001) was associated with patency loss at 1 month (Table 2A), and age and operation were associated with 1-year patency loss (Table 2B; Age ≥ 70 years, OR 3.86, p=0.004; DP, OR 4.66, p=0.014).
ConclusionAttention to intraoperative reconstruction technique is essential to optimize mesoportal venous patency. Techniques prioritizing native vein preservation are associated with the highest patency rates and are preferred when the tumor-vein interface permits. When SVL or more complex reconstructions are required, measures to mitigate the increased risk for patency loss should be considered. While initial consideration should be given to TR or SR with primary anastomoses, when concern for venous involvement exists, the safest reconstruction technique should be utilized.
Back to 2024 Abstracts


