Back to 2024 Abstracts
ANALGESIC EFFICACY OF ERECTOR SPINAE PLANE BLOCK IN LAPAROSCOPIC ABDOMINAL SURGERIES: A SYSTEMIC REVIEW AND META-ANALYSIS
Gabrielle Eloise Koh*, Crystal Sia
1, Sheila Wee
2, Angie Phui Sze Au Yong
3, sui an lie
3, Winson Tan
1, Fung Joon Foo
1, Juinn Huar Kam
1, Daniel Lee
2, Frederick H. Koh
11Sengkang General Hospital, Singapore, Singapore; 2Khoo Teck Puat Hospital, Singapore, Singapore; 3Singapore General Hospital, Singapore, Singapore
IntroductionEnhanced Recovery after Surgery (ERAS) protocols are rapidly becoming the standard of care for patients undergoing elective surgery with aims to expedite post-operative recovery and decrease morbidity. Multimodal analgesic therapy is a major cornerstone of ERAS and encompasses oral analgesics, patient-controlled analgesia (PCA), and locoregional anaesthetic techniques such as interfascial plane blocks (IPB). IPB first came into the limelight with the introduction of the transversus abdominis plane block technique in 2001. In comparison to other IPB techniques, ESPB stands out because of its relative simplicity, ability to provide both somatic and visceral analgesia with a single level injection and optimal safety profile. Despite its benefits, widespread adoption of ESPB has yet to gain significant traction.
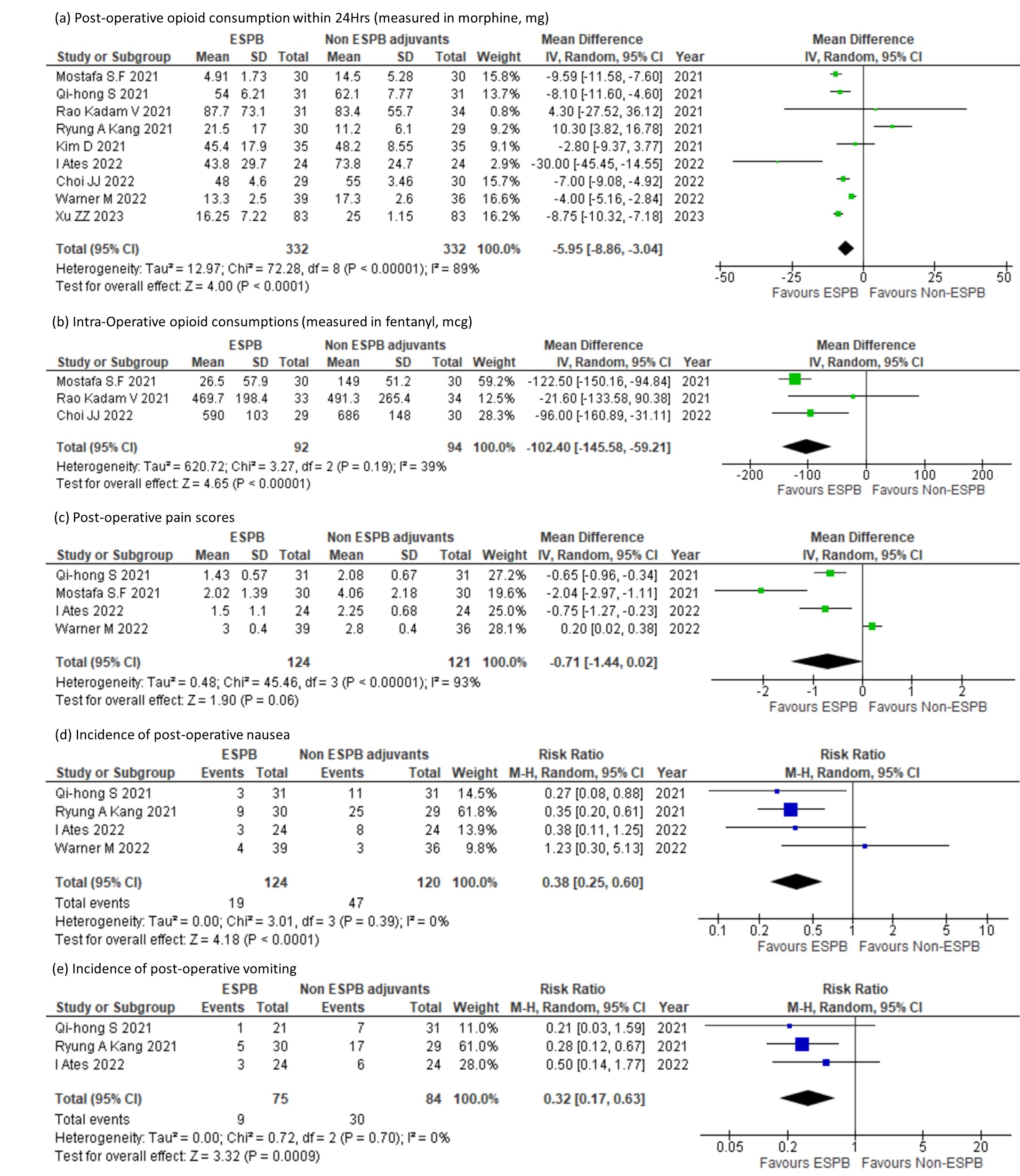
This study aims to review the efficacy of the ESPB as an adjuvant analgesia in laparoscopic surgeries – with exclusion of day surgery procedures such as laparoscopic cholecystectomy. The primary outcome is post-operative opioid consumption. Secondary outcomes are intra-operative opioid consumption, post-operative pain scores and incidences of nausea, vomiting.
MethodsThe literature search retrieved 1540 citations. 9 studies with 666 participants were eventually included in the meta-analysis.
ResultsThe pooled effects of the 9 RCTs revealed that ESPB significantly reduces the opioid demand within the first 24 hours post-operatively [mean difference (MD) of -5.95mg (95% CI: -8.86 to -3.04;
p< 0.00001)]. Similarly, patients that received ESPB had a lower intra-operative opioid requirement [MD of -102.4mcg (95% CI: -145.58 to -59.21;
p< 0.00001). In terms of post-operative complications, ESPB was further associated with a lower risk of developing post-operative nausea [RR 0.38 (95% CI: 0.25 to 0.60;
p<0.0001)] and vomiting [RR 0.32 (95% CI: 0.17 to 0.63;
p=0.0009)]. ESPB did not significantly reduce post-operative pain scores [MD of -0.71 (95% CI: -1.44 to 0.02;
p=0.06)].
Conclusion This meta-analysis demonstrated that in patients undergoing laparoscopic abdominal surgery, ESPB may benefit recovery by reducing peri-operative opioid consumption, and incidence of nausea and vomiting. However, post-operative pain scores did not differ significantly when all surgeries were analysed together. Nonetheless, while the Visual Analogue Scale attempts to objectify pain which is a subjective experience, it is still vulnerable to inter and intra-individual variability. This may be attributed to concomitant physical, physiological and psychosocial factors that can confound the actual experience of 'pain'.
This pooled analysis validates the efficacy of ESPB as an adjuvant analgesia in laparoscopic surgeries. Along with its favourable side effect profile and ease of administration, ESPB proves to be a promising adjunct for multimodal analgesia.
Back to 2024 Abstracts


