Back to 2024 Abstracts
ASSESSMENT OF STANDARD AND NOVEL HIGH RESOLUTION MANOMETRIC CHARACTERISTICS AFTER MAGNETIC SPHINCTER AUGMENTATION: A COMPENSATORY INCREASE IN CONTRACTILITY IS REQUIRED TO MAINTAIN BOLUS CLEARANCE
Sven Eriksson
*1, Lubomyr Boris
1, Sarah Scott
1, Ping Zheng
1, Inanc Sarici
1, Blair Jobe
1,2, Shahin Ayazi
1,21Esophageal Institute, Department of Surgery, Allegheny Health Network, Pittsburgh, PA; 2Department of Surgery, Drexel University College of Medicine, Philadelphia, PA
Introduction: Magnetic sphincter augmentation (MSA) of the lower esophageal sphincter (LES) has ramifications for esophageal body function. There is debate on whether increased postoperative esophageal contractility is improved motility secondary to resolution of reflux or compensation for increased outflow resistance at the esophagogastric junction. Assessment of novel high-resolution impedance manometry (HRIM) characteristics may provide insight into this debate. The aim of this study was to assess the impact of MSA on novel and standard HRIM characteristics.
Methods: Patients with no dysphagia after MSA were approached for HRIM one year after surgery. Pre- and postoperative HRIMs were reanalyzed. Novel HRIM characteristics included transition zone (TZ; length between distal end of skeletal muscle and proximal end of smooth muscle contractile waves), proximal latency (PL; time between swallow and smooth muscle wave initiation) and peristaltic completion time (PCT; time between swallow initiation and the intersection of the distal esophageal contraction and LES). These and standard manometric characteristics were compared before and after surgery. Patients with and without ≥20% postoperative incomplete bolus clearance were also compared.
Results: The study population included 120 patients (63.3% female) with a mean (SD) age of 56.1(13). Manometry was repeated at 15.7(9) months after surgery (
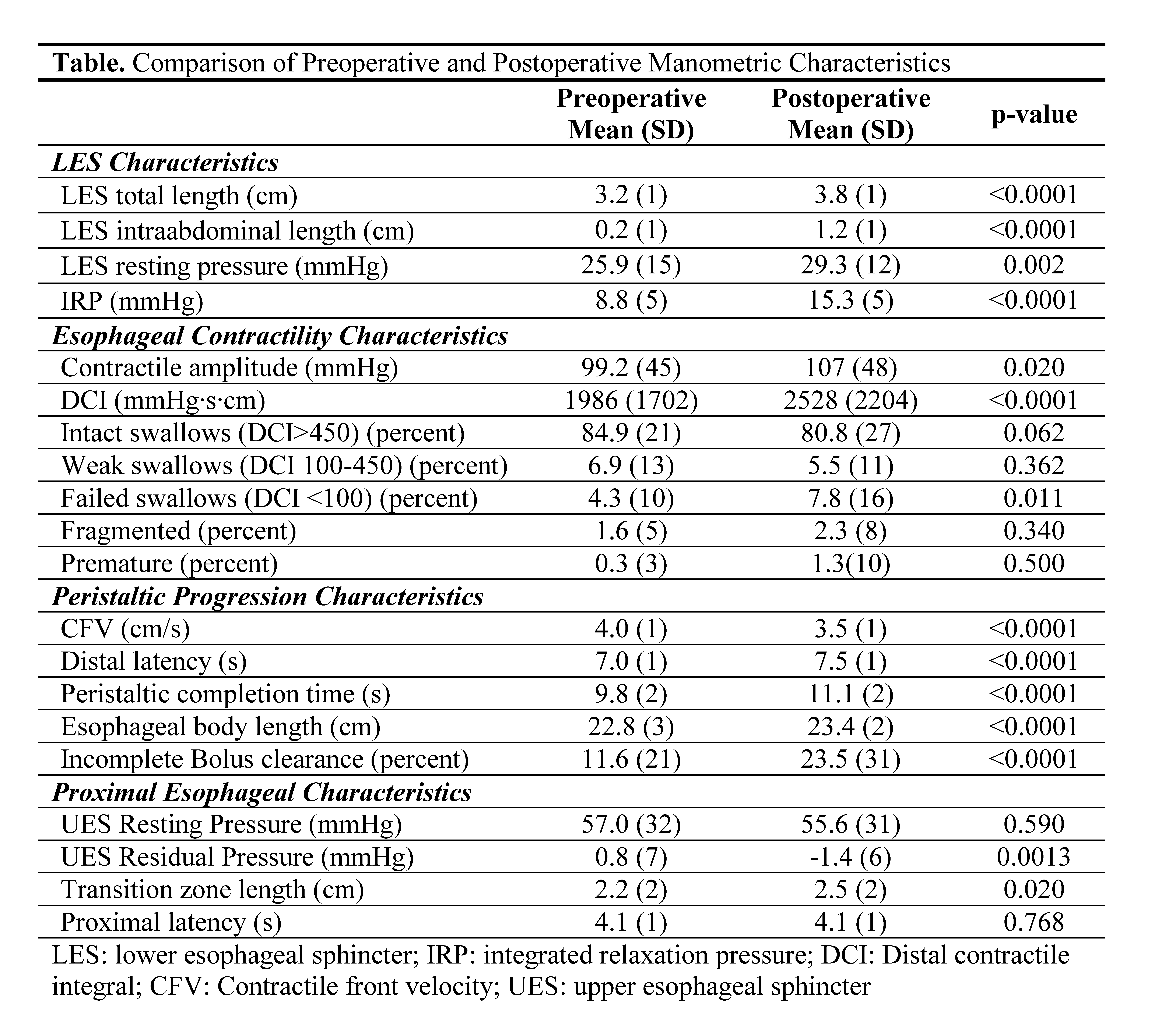
Table). MSA improved all LES resting characteristics (p<0.05). Integrated relaxation pressure (IRP) increased (p<0.001) and was associated with increased contractile amplitude (p=0.020) and distal contractile integral (DCI) (p<0.001). However, % failed swallows also increased (p=0.011) and was associated with worse incomplete bolus clearance (p<0.001). There was no change in PL (p=0.768), but after peristalsis initiated, progression was slower with decreased contractile front velocity (p<0.001) and longer DL (p<0.001) and PCT (p<0.001). Esophageal body length (p<0.001) and TZ length (p=0.020) increased.
There were 49 (40.8%) patients with ≥20% postoperative incomplete bolus clearance. Patients with poor clearance had a pre-post increase in incomplete bolus clearance [20.6(25) to 54.7(26) p<0.0001] and failed swallows [7.5(13) to 18.1(21), p<0.001], with no change in DCI (p=0.234) or MWA (p=0.116). By contrast, patients with >80% clearance had increased DCI [2164(1646) to 2958(2001), p<0.001] and MWA [108(47) to 125(48), p<0.001] with no change in bolus clearance (p=0.107) or percent failed swallows (p=0.084). Postoperative IRP was similar between groups (p=0.913).
Conclusions: MSA increases LES resting characteristics and IRP. Increased IRP induces a compensatory increase in esophageal body contractility to maintain bolus clearance in most patients. Patients who fail to generate this compensatory increase in contractility have poor bolus clearance.
Back to 2024 Abstracts


