
ILEAL POUCH ANASTOMOSIS ADVANCEMENT FOR THE TREATMENT OF POUCH-VAGINAL FISTULA
Michael Klingler*, Ipek Sapci, Amy L. Lightner, Scott Steele, Stefan D. Holubar, Tracy L. Hull
Digestive diseases and surgery, Cleveland Clinic and Foundation, Cleveland, OH
Introduction: Pouch vaginal fistulae (PVF) that develop after ileal pouch anal anastomosis (IPAA) can be difficult to manage. Circumferential IPAA pouch advancement (CPA) is a procedure that involves circumferentially dissecting the pouch-anal anastomosis above the level of the internal sphincter muscles via a perineal approach, allowing advancement of healthy tissue to re-anastomose. CPA has been previously described, although there are few published data on clinical outcomes following this procedure. We aimed to describe the indications and outcomes of CPA.
Methods: Patients with IPAA who underwent CPA for any indication between Jan 2009 and Jan 2021 were queried from a clinical database. Demographic variables were collected, and technical aspects of the IPA procedure were assessed via operative reports. An early fistula was defined as occurring <1 year after IPAA creation, whereas late fistulas were those that developed any time ?1 year. Clinical success was defined as resolution of the symptoms necessitating CPA with no stoma at the time of follow up. Patients who underwent pouch advancements with less than a full circumferential dissection, or other procedures such as pouch advancement flaps, were excluded. Patients with <3 month follow up were also excluded.
Results: Thirty-two potential patients were identified via EMR inquiry: 26 patients had procedures other than CPA and were excluded, leaving 6 in the final analysis. The average age at IPAA and CPA was 27.8 ± 5.9 years and 35.5 ± 9.1 years, respectively. The indication for CPA was a pouch vaginal fistula in all six patients. Three patients developed an early PVF and three developed a late PVF after IPAA. The mean number of procedures aimed at repairing the PVF prior to CPA was 1.6 ± 0.74. All patients had the diagnosis of ulcerative colitis at the time of IPAA, and three of the six patients who developed late fistulae currently have the diagnosis of Crohn's disease. Three patients had a DLI already present at the time of surgery, two had a DLI constructed at the time of surgery, and one patient did not have a stoma at any point. Postoperative complications occurred in two patients, including high stoma output and a postoperative hematoma requiring operative intervention. Average follow up time after CPA was 15.2 ± 8.4 months. Four of the five patients with DLI had reversal at the time of follow up, and the average time to DLI reversal was 4.5± 1.2 months. Clinical success was achieved in three of six (50%) of patients at the time of last follow up.
Conclusions: Perineal CPA is an effective treatment for refractory pouch vaginal fistulae and may be a treatment option for patients who have had multiple attempts at fistula repair. Larger studies with longer patient follow up are needed to evaluate complication rates and long-term success.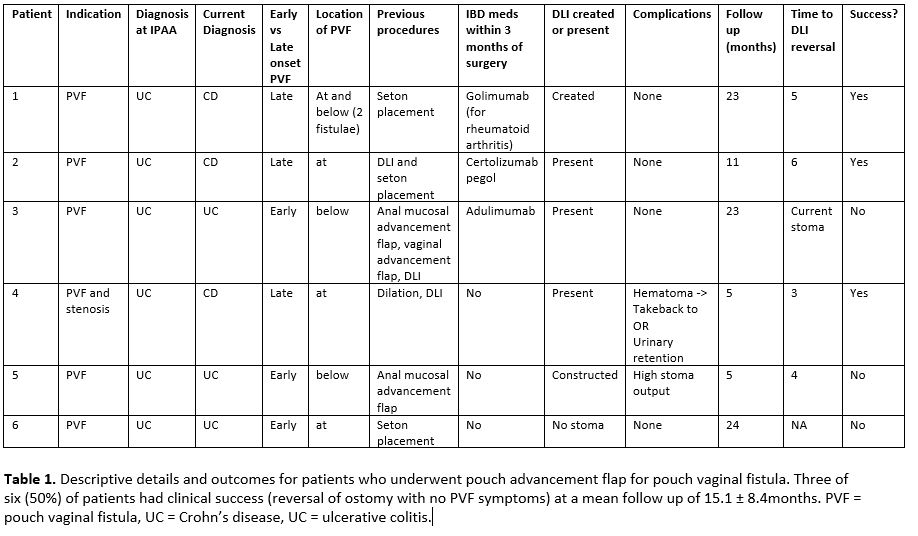
Back to 2022 Posters