
ASSOCIATION BETWEEN FACILITY VOLUME OR OPERATIVE APPROACH AND POSTOPERATIVE MORTALITY FOR RESECTED PRIMARY LIVER MALIGNANCIES
Jonathan J. Hue*, Kelly Hoerger, Mohamedraed Elshami, Richard S. Hoehn, Luke Rothermel, John Ammori, Jeffrey Hardacre, Jordan M. Winter, Lee M. Ocuin
General Surgery, University Hospitals Cleveland Medical Center, Univeristy Heights, OH
Introduction
Minimally invasive hepatectomy (MIS) is being performed in greater frequency for patients with hepatocellular carcinoma (HCC) and intrahepatic cholangiocarcinoma (ICC). The relationship between facility hepatectomy volume and postoperative mortality is undefined. We performed a comparative analysis of postoperative outcomes stratified by facility hepatectomy volume and operative approach.
Methods
The National Cancer Database (2010-2017) was queried for patients who underwent hepatectomy for localized HCC or ICC. Patients were grouped by operative approach (open v MIS [laparoscopic, robotic, or converted]) and stratified into tertiles based on total (?40, 41-80, ?81 cases), open (?40, 41-64, ?65 cases), and MIS (?24, 25-48, ?49 cases) facility volume over the study period. Subset analyses based on open and MIS approach were performed. The primary outcome was 90d mortality. We adjusted for clinicodemographic variables using multivariable logistic regression.
Results
A total of 14,492 patients were included: 78% had HCC and 22% had ICC. Most hepatectomies were minor (58%) and 73% were performed open. The overall 90d mortality rate was 7.2%. Major hepatectomy (8.6% v 5.9%, OR 1.55, p<0.001) and open hepatectomy (7.8% v 5.6%, OR 1.32, p<0.001) were both associated with an increased likelihood of 90d mortality compared to minor hepatectomy or MIS, respectively. Total facility volume ?40 cases was associated with higher 90d mortality as compared to 41-80 cases (10.0% v 6.7%, OR 1.49, p<0.001; Figure). Total facility volume ?81 cases was associated with a reduced likelihood of 90d mortality (5.4%, OR 0.81, p=0.04). Open volume ?40 cases was associated with an increased likelihood of 90d mortality as compared to 41-64 cases (9.9% v 7.1%, OR 1.28, p=0.04). Open facility volume ?64 cases was associated with a reduced likelihood of 90d mortality (6.0%, OR 0.79, p=0.07).
Among patients who underwent a MIS hepatectomy, major hepatectomy was associated with an increased likelihood of 90d mortality relative to minor (7.3% v 4.9%, OR 1.67, p=0.003). Treatment at facilities that performed ?24 MIS cases over the study period was associated with increased 90d mortality (7.2%, OR 1.99, p=0.003) relative to facilities that performed 25-48 MIS cases (3.9%). Facility volume ?49 cases was not associated with a reduced likelihood of 90d mortality (3.5%, OR 1.04, p=0.88)
Conclusion
Patients undergoing open hepatectomy for HCC or ICC are at increased risk of 90d postoperative mortality compared to MIS. Higher facility volume is associated with lower likelihood of 90d mortality for overall, open, and MIS hepatectomy. While causes of 90d mortality are unclear and likely multifactorial, these data are important when counseling patients on treatment options. Surgeons should consider the implications of institutional surgical volume when planning surgical approaches.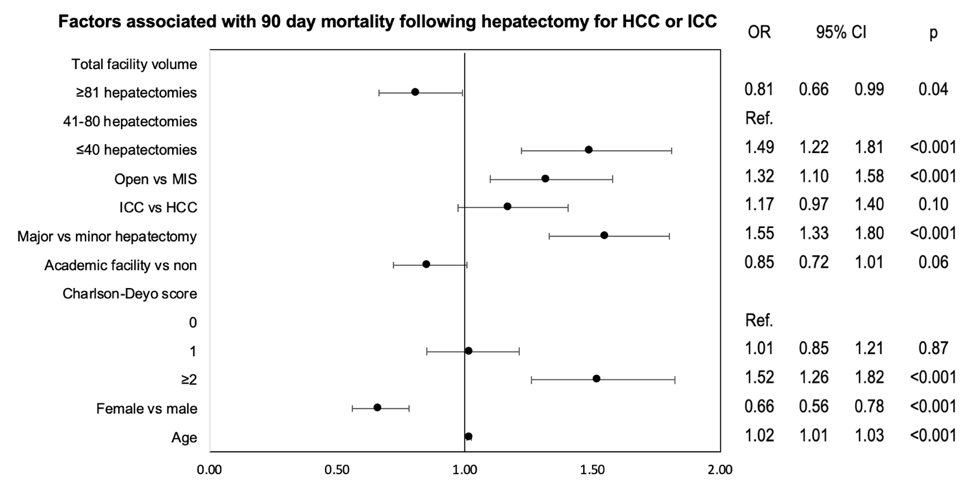
Back to 2022 Abstracts