
ENDOSCOPIC MANAGEMENT OF PATIENTS WITH A T-PROBE.
Karina Flores Marín, Roberto Delano-Alonso*, Carlos Valenzuela-Salazar, Roberto A. Garcia Manzano, Jose J. Herrera-Esquivel, Mucio Moreno Portillo, Stephania Medina González, Maria F. Morales Jiménez
Endoscopia Gastrointestinal, Hospital General Dr Manuel Gea Gonzalez, Ciudad de Mexico, Ciudad de México, Mexico
INTRODUCTION: In choledocholithiasis, the initial treatment must be endoscopic, surgical exploration is reserved for those who have not been resolved endoscopically. The surgical exploration of the bile ducts continues to be performed by open approach in various institutions, therefore, the use of T-probes continues in force at this time. Specific management of complications and pathologies associated with the use of a T-probe is required.
OBJECTIVE: To describe the use of endoscopy as a tool for the treatment and resolution of complications and pathologies associated with the use of a T-probe in biliary pathology.
MATERIAL AND METHODS: Observational, descriptive and retrospective study including demographic variables (sex, age, gender), pathology that merited a T-probe, reference diagnosis, type of endoscopic management and associated complications, diagnosis after endoscopic study.
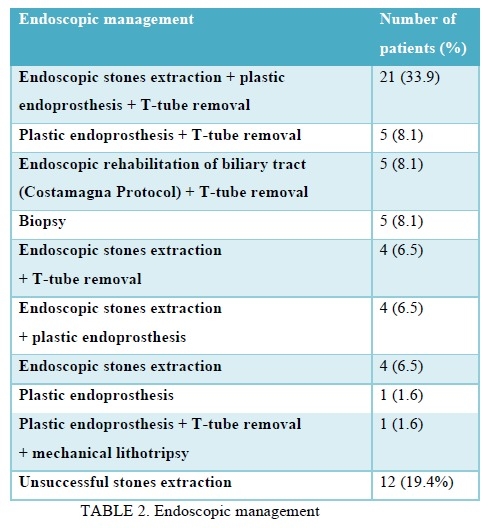
RESULTS: 62 records of patients with biliary T-probe from March 24th, 2015 to March 31st, 2021 were analyzed. Patients were referred from different hospitals throughout the country; 50 (81%) women with a mean age of 47 years. The main surgical procedure for which the T-probe was placed was open cholecystectomy with exploration of the bile duct for choledocholithiasis (n = 48), laparoscopic cholecystectomy with EDB (n = 10) and open cholecystectomy with suspected biliary lesion. (n = 4). The diagnoses after endoscopic study were 30 choledocholithiasis (48.4%), 5 neoplasms (8.1%) (4 ampulomas, 1 pancreatic head neoplasm), 4 bile leaks (6.5%), 3 biliary stenosis (4.8%), 2 biliary stenosis with biliary leakage (3.2%), 2 choledocholithiasis with cholangitis (3.2%), 1 choledocholithiasis with biliary leakage (1.6%) and hemobilia in 1 patient (1.6%). Two patients (3.2%) had complications. All pathologies associated with the use of a T-probe were 100% resolved endoscopically. The median number of interventions needed to completely resolve cases of choledocholithiasis, biliary stenosis and biliary leakage was 1.2.
CONCLUSION: The use of endoscopy as a tool for the treatment and resolution of complications associated with the use of T-probe in biliary pathology is a safe and effective option as described in this paper.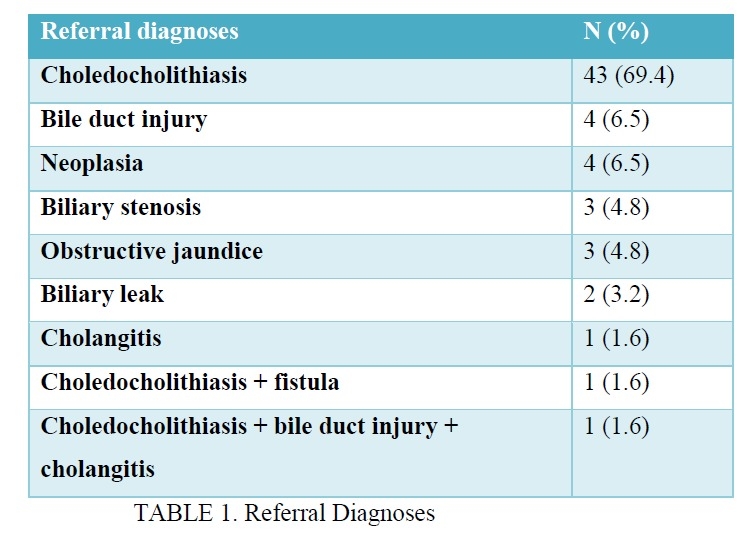
Back to 2022 Posters