
PREOPERATIVE CHEMOTHERAPY VERSUS UPFRONT SURGERY FOR STAGE CT4 GASTRIC CANCER: WHAT IS THE BEST STRATEGY?
André R. Dias, Marina A. Pereira, Marcus F. Ramos, Ulysses Ribeiro*, Bruno Zilberstein, Sergio Carlos Nahas
Universidade de Sao Paulo Instituto do Cancer do Estado de Sao Paulo, Sao Paulo, São Paulo, Brazil
Background: Stage T4 gastric cancer (GC) is the extreme in wall invasion, being a particularly challenging condition to manage. Although, combined modality therapy (CMT) with chemotherapy followed by surgery is recommended in advanced GC, T4 lesions usually undergo upfront surgery, since lesions are symptomatic with bleeding and outlet obstruction. At this time, due to the paucity of data and its low quality, it is unknown if preoperative CMT is a better strategy than upfront surgery in T4 GC.
Objective: Therefore, this study aimed to evaluate the best strategy in cT4 GC (preoperative CMT vs. upfront surgery).
Methods: Patients with gastric adenocarcinoma staged as cT4, who underwent gastrectomy with curative intent were included. Patients were divided according to initial treatment: upfront surgery (SURG) or chemotherapy + surgery (CMT+SURG). Primary outcome was overall survival (OS). Preoperative CMT was considered a dichotomous variable (received or not), regardless of the regimen received or its intention (neoadjuvant, perioperative, conversion).
Results: Of 1,330 GC operated, 685 received potentially curative surgery. Of these, 266 were initially staged as cT4: 150 underwent SURG and 76 CMT+SURG. In the SURG group, 95 received adjuvant CMT. Both groups were similar concerning age, comorbidities, ASA, hemoglobin, albumin, type of gastrectomy and lymphadenectomy performed. The CMT+SURG group had fewer metastatic lymph nodes and less advanced pTNM. The 30-day mortality in SURG and CMT+SURG was 5.3% and 2.6%, respectively (p=0.35). Median OS was 32 and 58.5 months for SURG and CMT+SURG, respectively (p=0.04). Those who had received perioperative or adjuvant CMT (n: 174) had better OS compared to surgery alone (49.4 vs 15.9 months, p<0.001). Median disease-free survival (DFS) for those with surgery alone was poor (4.5 months). OS was similar for those receiving preoperative and adjuvant CMT. Absence of CMT, pN+ and R1 resection were independent risk factors for lower OS.
Conclusion: Multimodal treatment (MMT) associating CMT with surgery, regardless of whether the approach is pre or postoperative is essential to improve the prognosis of cT4 GC. As tolerance to adjuvant treatment is reduced, preoperative CMT assures that the patient receives MMT and is a better strategy for cT4 GC compared to upfront surgery.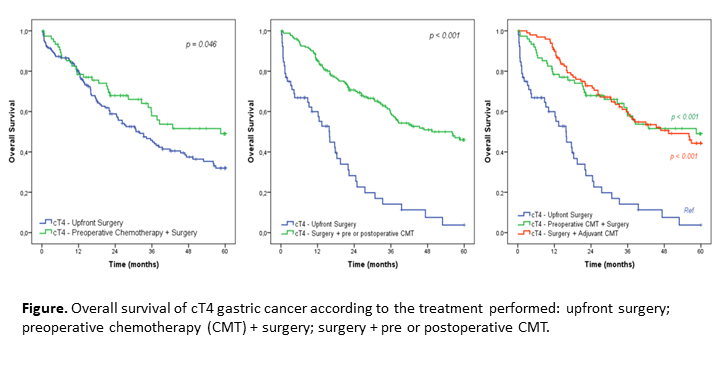
Back to 2022 Abstracts