
MIRIZZI SYNDROME TYPE IV ENDOSCOPY-ASSISTED APPROACH
Jesus I. Hernandez Solis*, Jose De Jesus Herrera Esquivel, Roberto Delano-Alonso, Adolfo Cuendis Velazquez, Jaime A. González-Angulo Rocha
Endoscopia Gastrointestinal, Hospital General Dr Manuel Gea Gonzalez, Ciudad de Mexico, Ciudad de México, Mexico
Mirizzi Syndrome (MS) is a rare pathology, it has been reported that only 0.1% of patients with gallstones will develop this condition 1 and of the four types described, type IV is the one diagnosed with the least frequency, with only 4% 2. The Csendes classification describes type IV as a cholecystobiliary fistula with a complete fusion of the gallbladder and the bile duct wall (BV) 3. The technique of choice to assess cholecystobiliary fistulas is the ERCP 4.
Case presentation:
A 57-year-old female with no significant history, who was admitted to our hospital due to high risk for choledocholithiasis and grade II acute cholangitis according to Tokyo 2018.
ERCP is performed where the dilated extrahepatic BV is observed with a maximum diameter of 30 mm in the proximal third and 21 mm in the distal third. Visualizing a filling defect in relation to a large stone with a diameter greater than 29 mm in the middle third of the common bile duct. Therefore, a plastic biliary prosthesis is introduced. Concluding study as endoscopically unresolved difficult choledocholithiasis secondary to large stone and massive dilation of extrahepatic BV.
Due to the size of the stone, it was decided to perform laparoscopic BV exploration, where a scleroatrophic gallbladder was visualized with involvement of more than two-thirds of extrahepatic BV.
Subsequently, intraoperative cholangioscopy is performed, introducing the endoscope through the subxiphoid port, locating choledochotomy, where free right and left hepatic ducts with slough epithelium are visualized.
In the second stage, the common bile duodenum anastomosis is carried out, verifying patency and tightness by intraoperative endoscopy. The evolution of the patient was favorable, with subsequent hospital discharge.
Conclusions:
The endoscopic approach assisted in BV explorations, performed in complex cases such as type IV MS, is a safe technique with good results. Highlighting the teamwork coordinated with endoscopic surgery and gastrointestinal endoscopy of our hospital.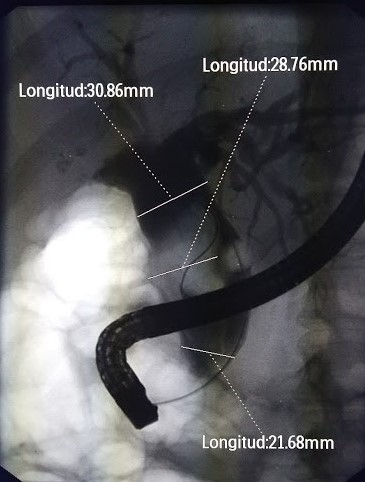

Back to 2022 Posters