
TOGETHER IS BETTER: PARTNERING OF ACADEMIC HOSPITALS WITH COMMUNITY HOSPITALS MAY BE THE ANSWER TO REGIONALIZATION OF CARE FOR ESOPHAGECTOMIES
Jessica Wu*, Tayler J. James, Shivani Sundaram, Jack Silva, Luke R. Putnam, Caitlin C. Houghton, Nikolai A. Bildzukewicz, John C. Lipham
Division of Upper GI and General Surgery, University of Southern California, Los Angeles, CA
Introduction:
Complex cancer surgeries have been a target for regionalization of care. Studies have shown outcomes of complex surgeries, including esophagectomies, are better at high-volume, academic centers. The purpose of this study was to assess the esophagectomy outcomes at an academic institution and its associated community hospital.
Methods:
A retrospective review of esophagectomies performed between 2010 and 2021 at an academic hospital and a community hospital was performed. The same surgeons operate at both institutions. Patient demographics, perioperative data, and outcomes were reviewed. Multivariable, stepwise logistic regression and Kaplan-Meier analyses were performed to compare outcomes between the two hospital systems.
Results:
A total of 198 esophagectomies were performed; 98 (49%) at the academic hospital and 100 (51%) at the community hospital. There were no differences in demographics or operative variables or immediate post-operative complications between the two groups (Table 1).
There were no significant differences in pre-operative cancer stage or cancer pathology between the two groups; however, more patients underwent neoadjuvant chemotherapy (72% vs 58%; P = 0.04) and radiation (61% vs 44%; P = 0.02) in the community group than the academic group. Though there were no differences in resection margins between the two groups, more lymph nodes were evaluated at the academic center (18 vs 21; P < 0.01).
Patients operated on at the community hospital experienced shorter stays in the intensive care unit (2 days vs 3 days; P < 0.01), but had a higher 30-day readmission rate at the compared to the academic center (10% vs 2%; P < 0.01).
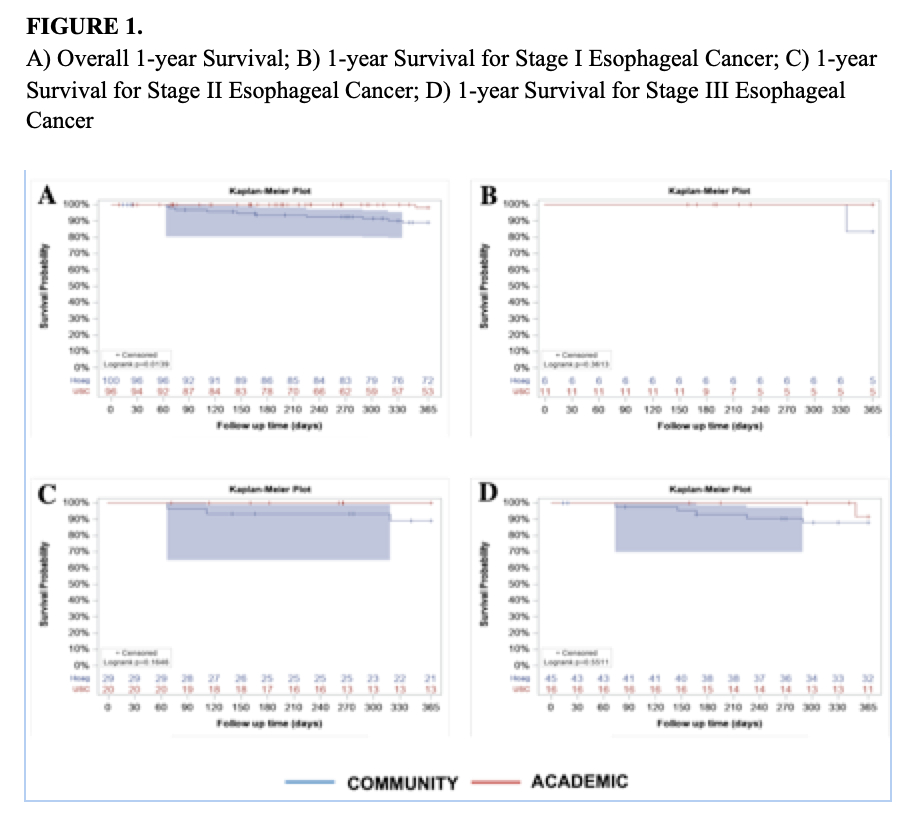
The 30-day mortality between the two groups was similar (0% vs 0%; P < 0.01). However, the academic center had a higher overall one-year survival rate than the community center (89% vs 98%; P = 0.01); however, there was no difference in one-year survival when stratified by pre-operative cancer stage (Figure 1).
Conclusions:
Outcomes after esophagectomy for cancer at an academic center and its affiliated community hospital were similar. Academic centers may consider partnering with community hospitals to provide complex cancer surgeries to a larger population and potentially mitigate the challenges to regionalization of care.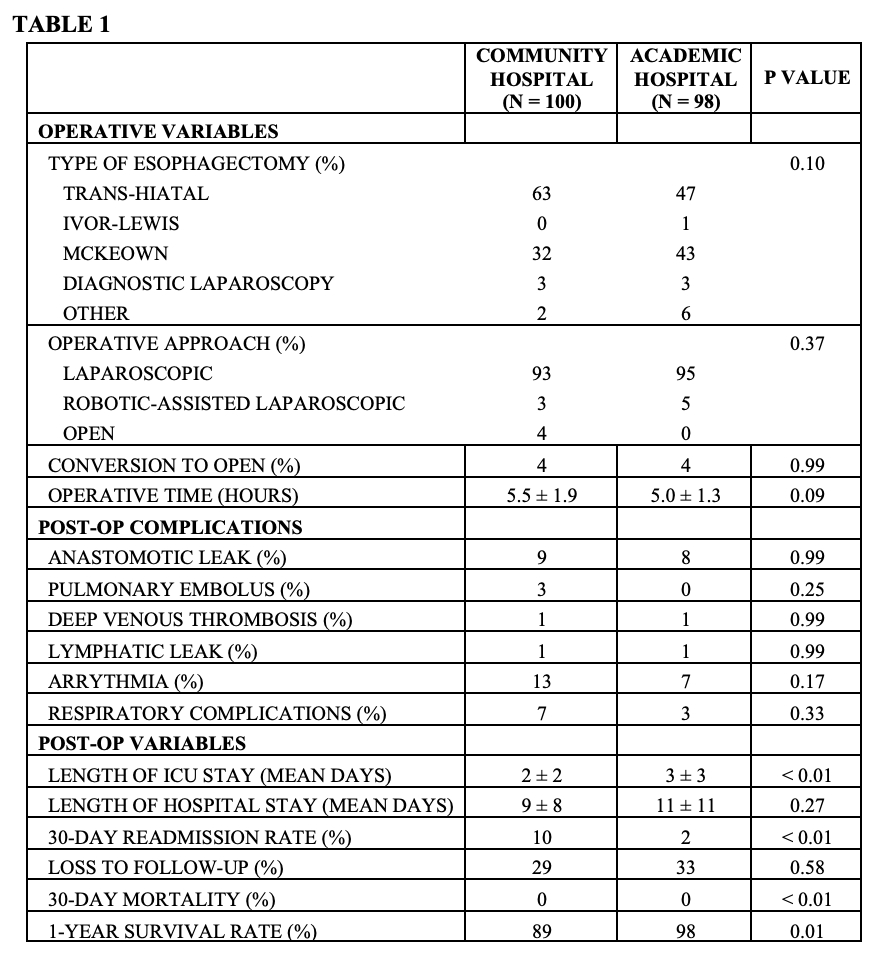
Back to 2022 Posters