
IS ENDOSCOPIC SUBMUCOSAL DISSECTION FOR COLORECTAL LESIONS PERFORMED IN THE ENDOSCOPY SUITE SAFE AND COST SAVING?
Cihad Tatar1, Ilker Ozgur1, Ipek Sapci1, Amit Bhatt2, David Liska1, Tracy L. Hull1, Scott Steele1, Emre Gorgun*1
1Department of Colorectal Surgery, Digestive Disease and Surgery Institute, Cleveland Clinic, Cleveland, OH; 2Department of Gastroenterology and Hepatology, Digestive Disease and Surgery Institute, Cleveland Clinic, Cleveland, OH
Background
Colorectal surgeons typically perform endoscopic submucosal dissection (ESD) in the operating room (OR) due to risk of procedural complications, including perforation. We hypothesized that, with increasing experience, it would be safe, feasible, and cost saving to select patients to perform ESD in the endoscopy suite (ES) rather than the OR.
Methods
The study includes consecutive patients who underwent ESD by a single experienced surgeon at a tertiary referral center between 2013 and 2019. Procedures performed during the surgeon's learning curve (between 2011 and 2013) were excluded. We compared patients undergoing ESD in the OR (between 2013 and 2017) to selected patients undergoing ESD in the ES (between 2017 and 2019) for age, gender, BMI, polyp size, polyp location, final pathology, length of stay, perioperative complications, and total procedures charges which were presented as the actual mean value of total charges for ESD in ES or OR divided by the actual mean value of total charges for ESD in OR. All ESD procedures in the ES were under conscious sedation while patients in the OR had general anesthesia.
Results
During the study period, 163 patients underwent ESD in the ES and 73 patients in the OR. ES and OR cases were similar in age, gender, BMI, intra-procedural, and postoperative 30-day complications. ES cases had significantly greater polyp size, right-sided polyps, and shorter hospital stays, with similar en-bloc and margin-negative resection rates, without an increase in complications (Table 1). There were seven (9.5%) immediate complications in the OR group. Five patients had perforation at the resection site, and all of them underwent laparoscopic primary repair. Two patients required surgery due to incomplete retrieval of the polyps and underwent wedge resection. There were two perforations as immediate complications in the ES group. One patient was taken to OR for laparoscopic suturing, and the other perforation was managed with endoscopic clipping. Late complications occurred in 10 (6.1%) patients in the ES group and 4 (5.5%) patients in the OR group (Table 2). The overall cost ratio of ESD procedures in ES to OR was 47% (p<0.001).
Conclusion
Colorectal ESD procedures performed in the endoscopy suite have similar efficacy and safety as those in the operating room. Procedures performed in the ES were associated with a shorter length of stay and significant peri-procedural cost saving.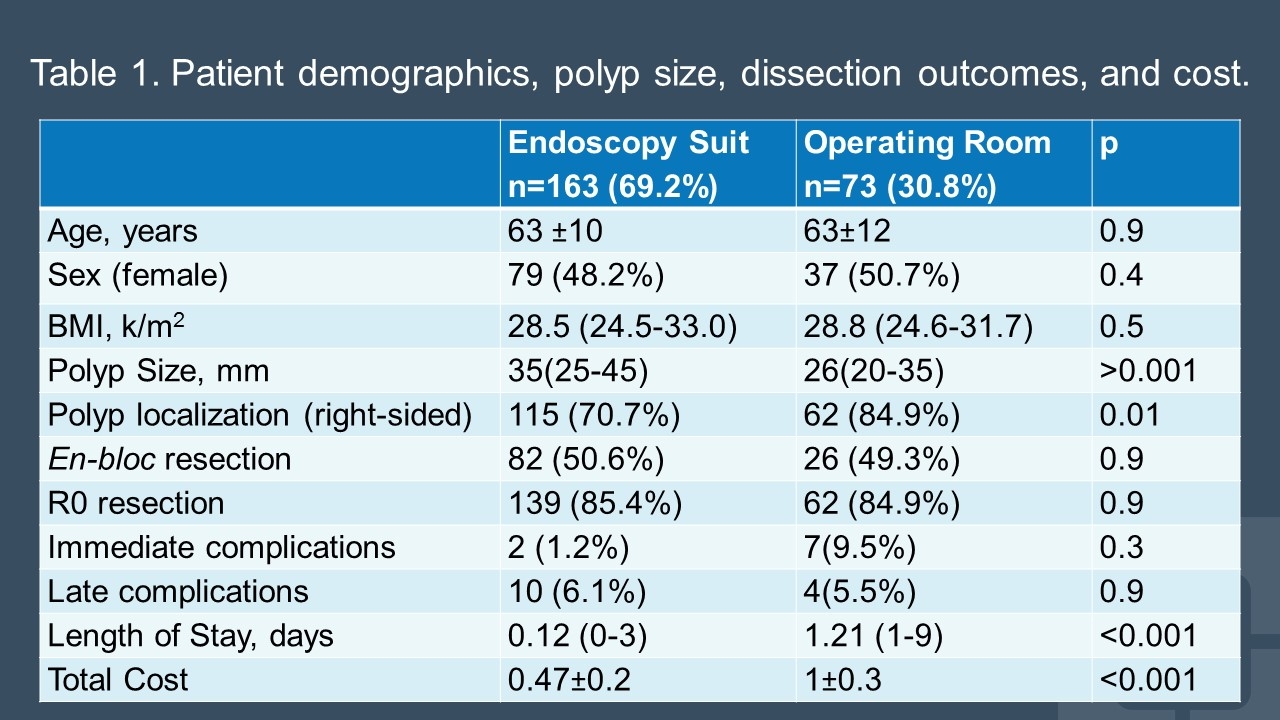
Table 1. Patient demographics, polyp size, dissection outcomes, and cost.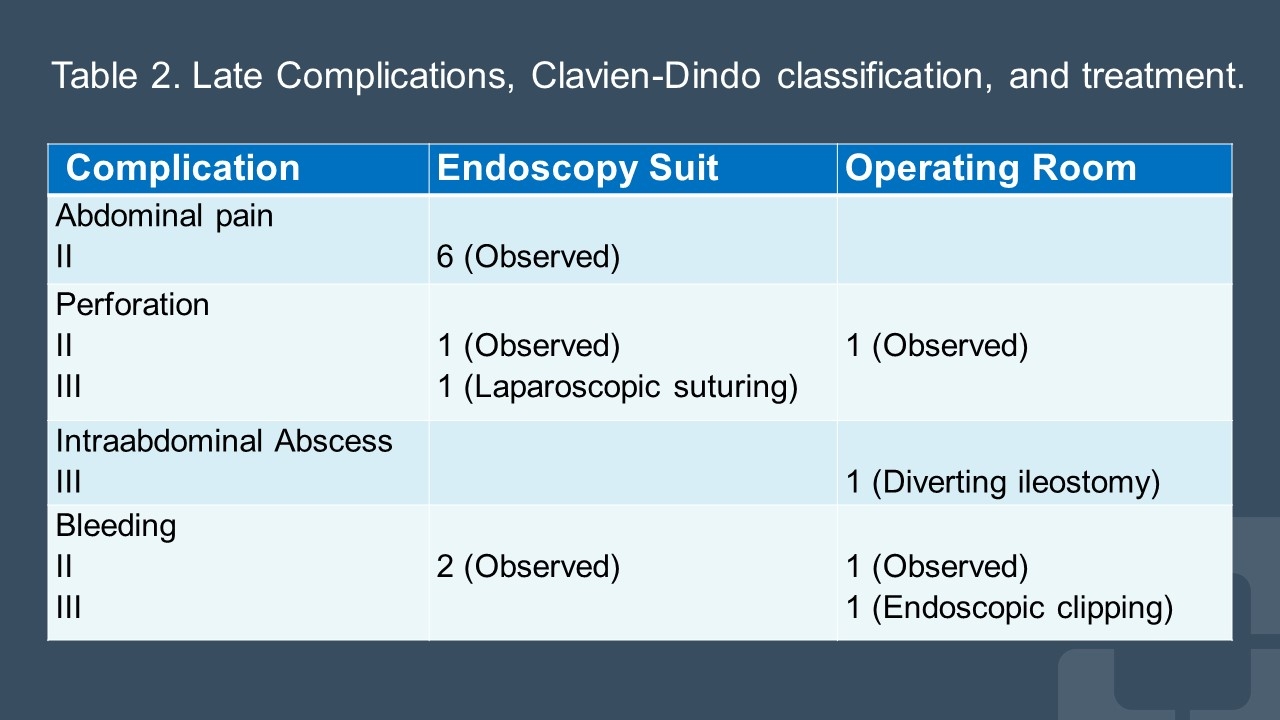
Table 2. Late Complications, Clavien-Dindo classification, and treatment.
Back to 2022 Posters