
RE-CONSTRUCTIVE TECHNIQUES FOLLOWING RESECTION OF MID AND LOW RECTAL CANCERS: AN UPDATED NETWORK META-ANALYSIS
Anvin Mathew*1, Deepti Ramachandra1, Anuj Goyal1, Mithun Nariampalli Karthyarth1, Gourav Kaushal3, Nirjhar R. Rakesh1, Abhishek Agrawal1, Princy M. Joseph2, Puneet Dhar1
1Surgical Gastroenterology, All India Institute of medical sciences, Rishikesh, Uttarakhand, India, Rishikesh, Uttarakhand, India; 2National Heath Systems Resource Centre, New Delhi, New Delhi, India; 3All India Institute of Medical Sciences - Bathinda, Bathinda, Punjab, India
Background
Following resection of mid and low rectal cancers, reconstruction options are Straight end-end Colorectal/anal Anastomosis (SCA), Colonic J pouch (CJP), Side-End Anastomosis (SEA), and Transverse Coloplasty (TCP). Many RCTs were comparing one to another published to date. Hence, we did a network meta-analysis to rank the techniques.
Background Evidence: As per the latest meta-analysis in 2015, CJP is superior to SCA for one year in functional outcomes. SEA and TCP have equivalent outcomes that of CJP, so indirectly, both are superior to SCA. Surgical outcomes were similar.
Methods
We included randomized trials that reported at least one functional or surgical outcome with the availability of at least six months of follow-up data. Functional outcomes were measured in three times frames, short-term (0- 8 months), Intermediate-term (9-18 months), long term (more than 18 months). Odds ratio (OR) and standardized mean difference (SMD) were used as pooled effect size measures. Frequentist model network meta-analysis was done
Results
Thirty-four trials (3072 patients) were included. Overall, 1312 patients (42.7%) underwent CJP, 861(28%) patients SCA, 476(15.5%) patients SEA, and 423(13.8%) patients TCP. CJP has less stool frequency that is seen in short [SMD=-2.05,95% CI= -2.80; -1.32] and intermediate-term [SMD=-0.8098, 95% C.I.=-1.5; -0.12] compared to SCA. Both SEA [SMD=-2.0, 95% CI= -3.11; -0.91] and TCP [SMD=-2.1, 95 % C.I.= -3.35; -1.05] maintained low stool frequency at short term, but the advantage was not maintained further. In short term CJP has better incontinence score compared to SCA [SMD= -1.17; 95% C.I.=-2.02; -0.32] so in intermediate term [SMD= -0.5616, P= 0.08]. SEA and TCP show no significant advantage in incontinence scores in any time frame. Patients undergoing SEA and TCP tend to use anti-diarrheal drugs more even in the long term, while CJP patients do not. TCP and SEA patients had more sensation of incomplete evacuation in the short term. On qualitative synthesis, Quality of Life (QoL) was better with CJP in the short term compared to SCA. CJP and SEA faired equally to CJP. TCP is at higher risk of an anastomotic leak [OR 11.9436; P= 0.0005] and anastomotic stricture [OR: 3.2072; P= 0.0120]. CJP, SEA, and SCA have equivalent leak and stricture rates. Urinary complications and SSI are significantly high with all CJP, SEA, and TCP. Pulmonary complications and peri-op mortality do not differ among groups.
Conclusion
Colonic J Pouch (CJP) should be the preferred reconstructive method following resection of mid and low rectal tumors owing to superior functional outcomes compared to other three reconstructive methods. Transverse Coloplasty(TCP) associated with increased anastomotic leak and stricture rate; hence should be used judiciously.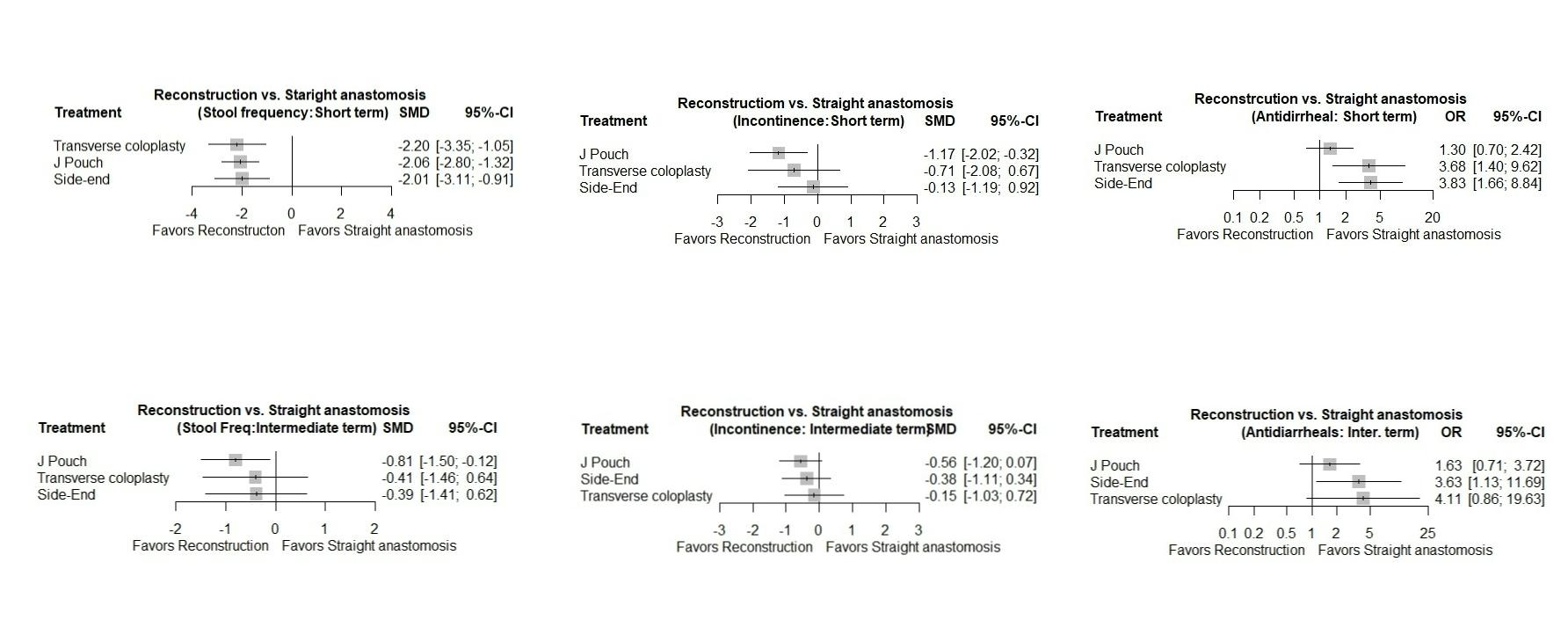
Functional Outcomes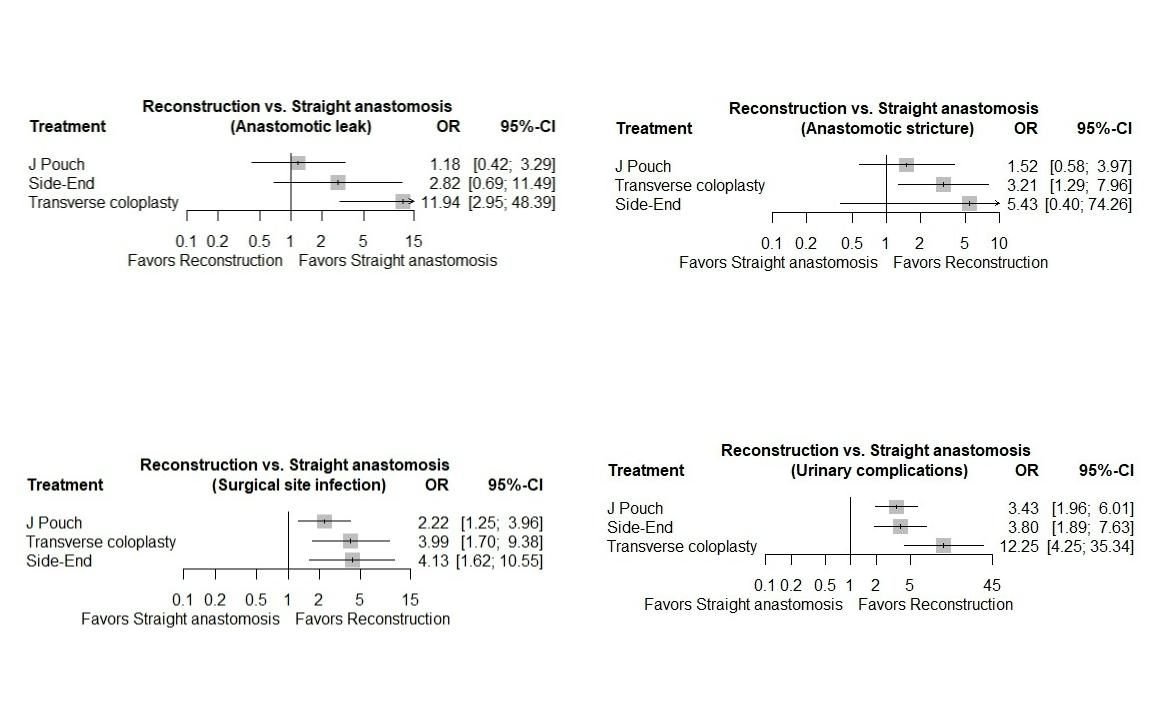
Surgical Outcomes
Back to 2022 Abstracts