
THE 5-FACTOR MODIFIED FRAILTY INDEX IS A PREDICTOR OF POSTOPERATIVE MORBIDITY IN PATIENTS UNDERGOING PERINEAL PROCTOSIGMOIDECTOMY
Dakota T. Thompson*, Jeremy Chang, Dana van der Heide, Mohammed O. Suraju, Garett Steers, Irena Gribovskaja-Rupp, Jennifer Hrabe, Imran Hassan
Surgery, University of Iowa Hospitals and Clinics, Iowa City, IA
Introduction: Perineal proctosigmoidectomy (Altemeier's procedure) for full-thickness rectal prolapse is a well-tolerated procedure in elderly patients even with comorbidities. However, these patients are at risk for postoperative complications, and identification of modifiable risk factors can lead to mitigation strategies. The 5-factor modified frailty index (mFI-5) has been used to predict postoperative morbidity, but its utility in patients undergoing an Altemeier's procedure has not been reported. We hypothesized that the number of medical comorbidities as measured by mFI-5 would predict the incidence of postoperative complications. Therefore, the aim of this study was to determine factors associated with postoperative morbidity in patients undergoing an Altemeier's procedure.
Methods: The American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) database was queried for patients undergoing an Altemeier's procedure between 2010 and 2018. The mFI-5 is calculated by adding a point for the following five comorbidities: insulin-dependent or noninsulin-dependent diabetes, congestive heart failure, hypertension, chronic obstructive pulmonary disease or pneumonia, and dependent functional status at time of surgery. Patients missing data for these comorbidities were excluded. Postoperative surgical morbidity as defined by the Clavien-Dindo classification was the primary outcome of interest. Univariate and multivariate logistic regression analyses were performed to adjust for confounding variables.
Results: During the study period, 4,779 patients [median age 80 years (IQR 69-87)] underwent an Altemeier's procedure of which 11.0% had a postoperative complication. Of these patients, 28.5% had an mFI = 0, 48.1% had an mFI = 1, and 23.4% an mFI ? 2. Patients with frailty as measured by the mFI (p < 0.001), advanced age (? 80 years), ASA class ? 3, emergency operations, ascites, dialysis, preoperative wound infection, transfusion requirement, anemia, thrombocytopenia, and hypoalbuminemia (all p < 0.05) had a higher incidence of complications. After adjusting for available confounders an mFI-5 of ? 2 (OR 1.43, 95% CI [1.00-2.03], p = 0.049) and other preoperative comorbidities were associated with increased postoperative complications, but advanced age (? 80 years) was not found to be an independent risk factor. (Table)
Conclusion: A proportion of patients undergoing an Altemeier procedure experience postoperative complications predicted by the mFI and other medical comorbidities but not age. These data suggest that physiological status is more relevant than chronological age in determining morbidity after surgery. Preoperative optimization of this high-risk group of patients (mFI ? 2) may lead to further decrease in perioperative complications and improved patient outcomes after an Altemeier's procedure.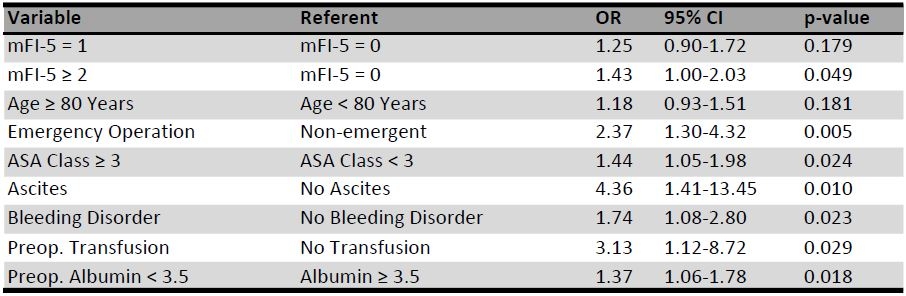
Table: Multivariate analysis of factors associated with any morbidity
Back to 2022 Posters