
VOICE HOARSENESS WITH REFLUX AS A SUSPECTED ETIOLOGY: INCIDENCE, EVALUATION, TREATMENT, AND SYMPTOM OUTCOMES
Sydney Korsunsky*, Leonel Camejo, Diep Nguyen, Rahul Mhaskar, Joel Richter, Joy Gaziano, Vic Velanovich
Surgery, University of South Florida, Tampa, FL
Background: Laryngopharyngeal reflux (LPR) as a cause of voice hoarseness remains a vexing diagnosis for providers with little consistency in best practices for evaluation and treatment. The purpose of this study was to describe the clinical evaluation course of patients with a primary complaint of hoarseness with suspected LPR, treatments received, rates of voice symptom improvement, and incidences of final etiologies of hoarseness.
Methods: A retrospective chart review was conducted of patients with a primary complaint of voice hoarseness with LPR as suspected etiology between October 2011 and March 2020 who underwent clinical evaluation, treatment, and follow-up. Data collected included if patients underwent endoscopy, barium swallow, esophageal pH-monitoring, esophageal manometry, and videostroboscopy. Treatments recorded included medical management (MM), surgical management (SM), and voice therapy/vocal hygiene techniques (VT). Symptom outcome was recorded from subjective report on patient charts. The evaluation and treatment period was determined as the interval between first and final visit. The final diagnosis was recorded from final visit charts.
Results: A total of 134 patients met inclusion criteria. Some patients underwent multiple diagnostic procedures. Videostroboscopy was the most common procedure (n=59, 44%) followed by endoscopy (n=38, 28%), pH-monitoring (n=28, 21%), manometry (n=25, 18%), and barium swallow (n=18, 13.4%). Most patients received solely MM (n=93, 69.4%), including protein pump inhibitors, H2-blockers, oral/nasal steroids, antihistamines, and vocal cord botulinum toxin injection. Treatment for 29 patients included VT (21.6%). Thirteen patients received SM (9.7%) including anti-reflux surgery and vocal cord procedures. The mean evaluation and treatment period for all patients was 16.1 months (median 8.63; range 0.2-72). The most common final diagnosis was gastroesophageal reflux disease (GERD) (25.37%), followed by multifactorial causes (17.16%) and dysphonia with unclear etiology (12.69%) (Table 1). Among all patients, 83 (61.9%) reported symptom improvement. A total of 28 patients were diagnosed with LPR or LPR with GERD (21%), and 22 reported symptom improvement (78.57%).
Conclusion: LPR as suspected etiology of voice hoarseness remains a difficult diagnosis to establish and represents a narrow group of patients with voice complaints. There is a wide variety of diagnostic techniques used for evaluation with no standardization of diagnostic criteria. Despite varying and inconsistent treatment modalities, most LPR and LPR with GERD patients improve over a year. There may be no further benefit to extra work-up for hoarseness as a primary complaint, especially in patients with LPR. Further studies should explore diagnostic criteria for LPR and the necessary and efficient clinical evaluation to establish a diagnosis.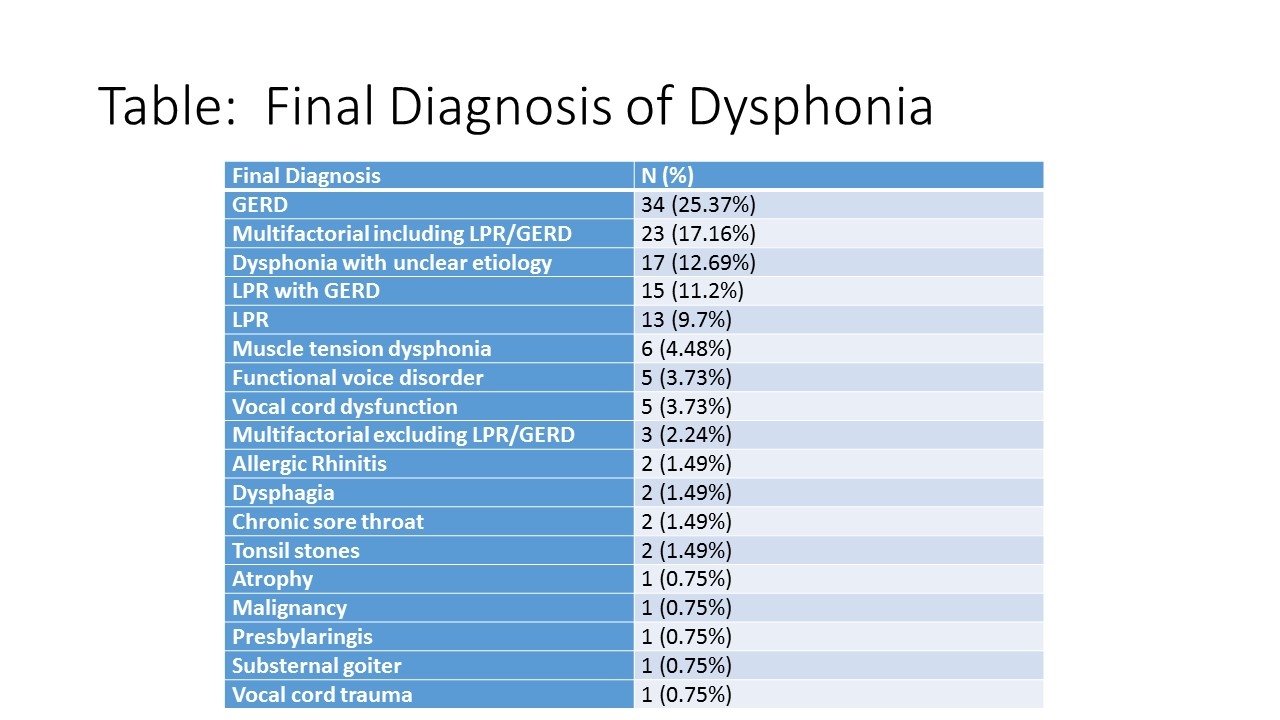
Back to 2022 Abstracts