
SAFETY AND FEASIBILITY OF OUTPATIENT RIGHT COLECTOMY FOR COLON CANCER
Sophia Y. Chen*, Shannon N. Radomski, Miloslawa Stem, Brian D. Lo, Bashar Safar, Jonathan Efron, Chady Atallah
Johns Hopkins Medicine, Baltimore, MD
Introduction:
Hospital length of stay (LOS) has been increasingly used as a surgical quality metric. Implementation of minimally invasive surgery, Enhanced Recovery After Surgery (ERAS) pathways, and multimodal analgesia with early discharge after colorectal surgery have been found to be safe with no increased rate of readmissions. The purpose of this study was to determine the safety and feasibility of right colectomy as an outpatient procedure for patients diagnosed with primary colon cancer.
Methods:
Using the American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) database and its associated Procedure Targeted Colectomy database (2016-2019), patients ?18 years of age diagnosed with colon cancer who underwent right colectomies were identified. Patients were categorized into four LOS groups: LOS ?1 day (outpatient), LOS 2-4 days, LOS 5-6 days, and LOS ?7 days. The primary outcomes were overall and serious morbidity. Secondary outcomes were mortality, readmission, and anastomotic leak. The association between LOS and overall and serious morbidity was explored using multivariable logistic regression.
Results:
16,646 adult patients were identified, of which 279 patients (1.7%) underwent an outpatient right colectomy. Compared to patients with a longer LOS, patients undergoing outpatient surgery were generally younger, with fewer comorbidities. Overall morbidity for the outpatient group was 7.5%, compared to 11.2%, 23.4%, and 41.8% for the LOS 2-4 days, LOS 5-6 days, and LOS ?7 days groups, respectively (p<0.001). There were no differences in the rates of anastomotic leak, mortality, and readmission in the outpatient group when compared to patients with LOS 2-4 days (anastomotic leak: 1.1% vs. 0.9%, p=0.744; mortality: 1.1% vs. 0.5%; p=0.180; readmission: 10.0% vs. 7.3%, p=0.087). The most common reason for readmission after outpatient right colectomy was ileus/bowel obstruction (32.1%). On multivariable analysis, there were no significant differences between patients with LOS ?1 day (ref) and LOS 2-4 days with respect to overall morbidity (OR, 1.50; 95% CI, 0.93-2.40; p=0.096) and serious morbidity (OR, 0.87; 95% CI, 0.44-1.71; p=0.680). However, patients with LOS ?5 days demonstrated increased odds of overall and serious morbidity (Table).
Conclusions:
Outpatient right colectomy is safe and feasible for a highly-select group of colon cancer patients, as there exists no increased odds of overall or serious morbidity compared to patients with a longer hospital LOS. Optimizing patients preoperatively and implementing targeted readmission prevention strategies may aid in selecting patients who are appropriate candidates for outpatient right colectomy.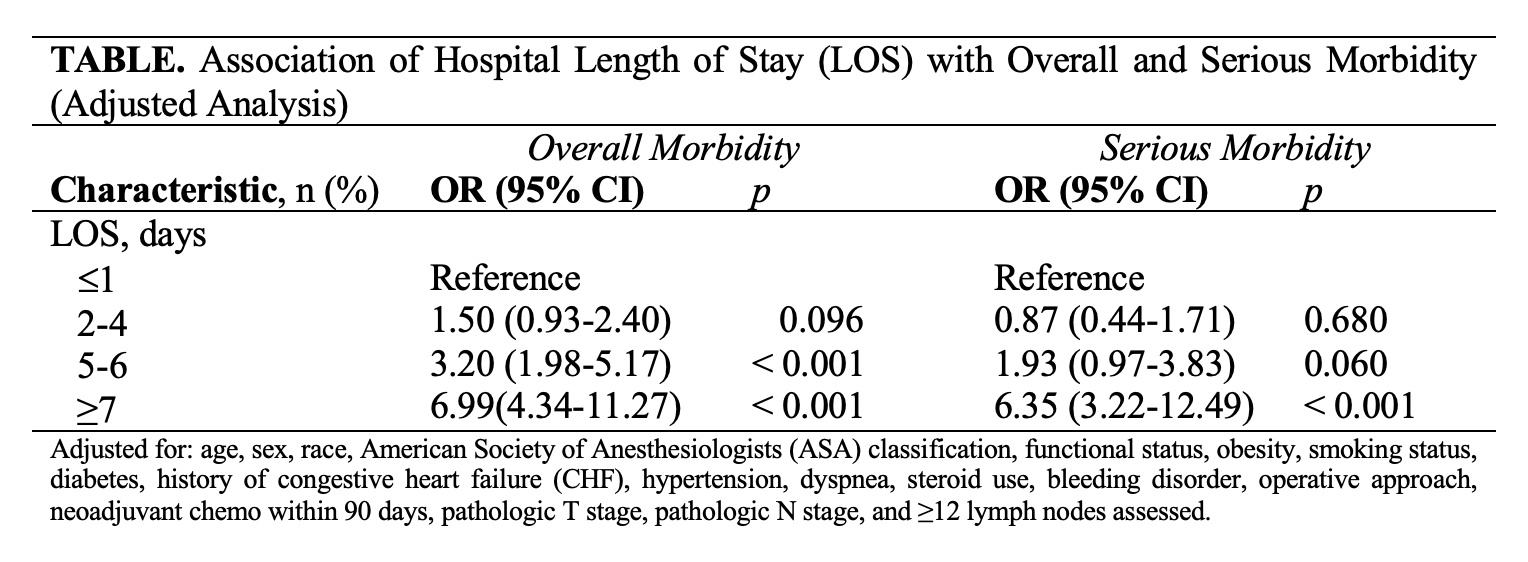
Back to 2022 Abstracts