
LONG-TERM EVALUATION OF AN ORIGINAL RADIOFREQUENCY HEMORRHOIDAL THERMOCOAGULATION PROCEDURE ON BLEEDING, PROLAPSE, QUALITY OF LIFE OF TREATED PATIENTS AND DURATION OF POSTOPERATIVE DOWNTIME IN A 5-YEAR SURVEY: "NO PAIN, NO GAIN" OR "NO PAIN BUT A GAIN"?
BENJAMIN RAUX3, ROMAIN DIDELOT2, FRANZ RUDLER2, AURELIEN MULLIEZ3, Anthony Buisson3, Armando Abergel3, Pierre Blanc2, JEAN-MICHEL DIDELOT*1,2
1Clinique Clementville, Montpellier, Languedoc-Roussillon, France; 2Universite de Montpellier, Montpellier, Languedoc-Roussillon, France; 3Centre Hospitalier Universitaire de Clermont-Ferrand, Clermont-Ferrand, France
Radiofrequency thermocoagulation (RFT) with transfixiant, not ball-shaped, probe is a newly proposed but poorly studied alternative technique to reduce pain and downtime after internal hemorrhoid surgery. After ethics committee approval, a retrospective monocentric study was done to assess efficacy of RFT on hemorrhoidal symptoms and quality of life (QoL).
RFT was not performed with anoscopy but by piercing exteriorized hemorrhoids at anal margin with electrode. A phone interview assessed evolution of hemorrhoidal prolapse rated by Goligher scale; bleeding and discomfort (0-10), sense of improvement and satisfaction (-5 to +5/5) by analog scales; impact of hemorrhoidal disease on QoL by validated HEMO-FISS-QoL score.
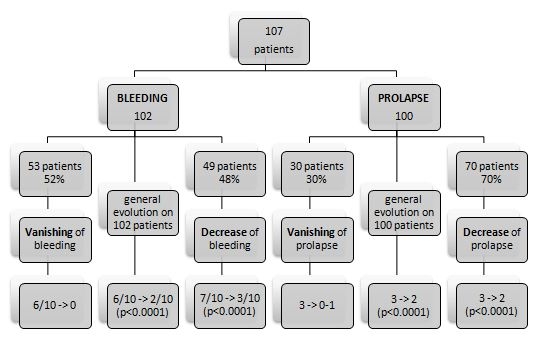
From April 2016 to January 2021, 124 patients were operated under general anesthesia and some data collected at postoperative visit 8 weeks later. In September 2021, 107 patients (75 men, mean age 54 years) could be interviewed (86%). Mean follow-up was 30 months (8-62). Over 86% were outpatients. Mean time off work was only 3 days, 71% resuming work the next day. Mean 4334 joules were applied. Of 102 patients, bleeding disappeared in 53 or dropped from 7 to 3/10 (p<0.001) in 49. 11 patients on anticoagulants before RFT had no postoperative hemorrhage nor more recurrent bleeding than without. Prolapse vanished in 30% of the 100 patients with preoperative grade 2 to 4 or reduced from mean grade 3 to 2 (p<0.001). External hemorrhoidal thrombosis was the only complication reported in 9 patients unrelated to used energy. Only 34% used stage II analgesics, none stage III. Hemorrhoidal discomfort fell from 7 to 2/10 (p<0.001). HEMO-FISS-QoL score improved from 22 to 7/100 (p<0.001). Sense of improvement and overall satisfaction remained high at +4/5. Of all patients, 92% would choose RFT again and 96% recommend it. Comparison to a previous study with only 15 months of survey shows maintenance of these positive results over time. 21% of patients reported recurrence in mean 22 months but only 6 required new surgery. When studied by Kaplan Meier curve, first operated patients differed from most recent ones for none of the studied postoperative criteria, including recurrence, suggesting an absence of learning curve.
The encouraging results of this long-term study with some of the highest number of patients and a longest follow-up published to date must be confirmed by randomized, multicentre prospective trials to position RFT in the management of internal hemorrhoidal disease. However, it shows that this new minimally invasive procedure allowing a rapid return to activity is very promising, significally improving QoL by eliminating or reducing bleeding and hemorrhoidal prolapse with few pain. It seems to be a very valuable reproducible technique, ideally suited for outpatient surgery, with high acceptance and low complications and recurring rates.
Back to 2022 Abstracts