
MITIGATING MORBIDITY IN OLDER PATIENTS UNDERGOING MAJOR PANCREATIC AND HEPATOBILIARY SURGERY
Seth Concors*1, Elsa M. Arvide1, Laura R. Prakash1, Tacara Soones2, An Ngo-Huang2, Vinh Q. Nguyen2, Timothy E. Newhook1, Naruhiko Ikoma1, Jessica E. Maxwell1, Hop Tran Cao1, Yun Shin Chun1, Michael P. Kim1, Jeffrey E. Lee1, Jean-Nicolas Vauthey1, Matthew Katz1, Ching-Wei D. Tzeng1
1The University of Texas MD Anderson Cancer Center Division of Surgery, Houston, TX; 2The University of Texas MD Anderson Cancer Center, Houston, TX
Background: National data have identified elevated rates of major morbidity after pancreatic and hepatobiliary surgery in older patients. In patients ?75yrs old, 90-day mortality is 12% after pancreatoduodenectomy (PD) in the National Cancer Database. Similarly, in large multi-center studies, 90-day mortality after hepatectomy is 8%. We hypothesized that multidisciplinary patient selection and optimization are associated with a reduction in expected age-related morbidity.
Methods: This is a retrospective cohort study of prospectively maintained data from consecutive pancreatectomies and hepatectomies at a single institution from July 2011-July 2021, and May 2017-May 2021, respectively. Multidisciplinary patient selection and optimization included consultation with prehabilitation, dietitian, and geriatric medicine when indicated for high-risk, functionally impaired, and/or older patients. We compared rates of 90-day postoperative morbidity between patients age ?49, 50-64, 65-74, and ?75.
Results: 1,353 pancreatectomies were performed (433 DP, 32.0%; 842 PD, 62.2% and 78 other/combination procedures, 5.8%), including 650 (48.0%) for pancreas adenocarcinoma. 462 (34.2%) and 153 (11.3%) patients were 65-74 and ?75, respectively. ACCORDION grade ?II and ?III complications occurred in 805 (59.5%) and 359 (26.5%) of patients, respectively, with 11 deaths (5 patients ?65). Age was not predictive of ACCORDION grade ?II or ? III complications after pancreatectomy (OR 0.92, 95% CI 0.81-1.03, p=0.17; OR 0.92, 95% CI 0.80-1.05, respectively) (Table 1).
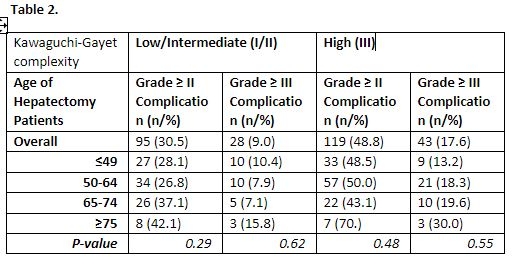
556 liver resections were performed, 326 (58.6%) for colorectal cancer, 55(9.9%) for cholangiocarcinoma, and 42 (7.6%) for hepatocellular carcinoma. 121 (21.8%) and 29( 5.2%) patients were 65-74 and ?75, respectively. ACCORDION grade ?II and ?III complications were seen in 214 (38.5%) and 71 (12.8%) of patients, respectively, with 3 deaths (1 patient ?65). When stratified by surgical difficulty (Kawaguchi-Gayet classification "low-intermediate" versus "high-risk"), high-risk procedures were associated with increased ?II grade complications (OR 2.2 95% CI 1.5-2.1, p<0.001) and ?III grade complications (OR 2.2, 95% CI 1.3-3.6, p<0.005). Age was not predictive of ACCORDION grade ?II and ?III complications when stratified by Kawaguchi-Gayet classification (p>0.1, Table 2).
Conclusions: Despite retrospective data from large national cohorts associating increasing age with greater complication rates, these differences were not seen in a single-institution dataset stratified by surgical extent. These data suggest, that with proper patient selection, routine prehabilitation, and preoperative physiologic optimization, the inherent morbidity associated with performing major operations on older patients can be mitigated.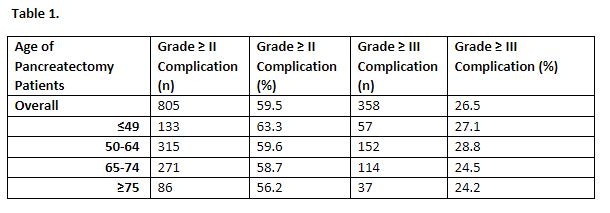
Back to 2022 Abstracts