
DECISION ANALYSIS COMPARING PREOPEATIVE ENDOSCOPIC SPHICTEROTOMY VERSUS IINTRAOPERATIVE ENDOSCOPIC SPHINCTEROTOMY VERSUS IINTRAOPERATIVE COMMON BILE DUCT EXPLORATION FOR THE MANAGEMENT CHOICE OF SUSPECTED CHOLEDOCHOLITHIASIS
Obada Kattih*, Vic Velanovich
Surgery, University of South Florida, Tampa, FL
Background The management of suspected choledocholithiasis remains a controversial issue. Choledocholithiasis can be suspected preoperatively, discovered intraoperatively during a laparoscopic cholecystectomy (LC), or identified post-LC as retained common bile duct (CBD) stones. At present, the three most common management options for choledocholithiasis include a preoperative endoscopic retrograde cholangiopancreatography (ERCP) with sphincterotomy (ERCP/ES) and stone extraction followed by LC, or a LC with intraoperative cholangiogram (LC/OIC), followed by either an intraoperative ERSP/ES or a laparoscopic common bile duct exploration (LCBDE). The purpose of this study was to assess the consequences of the decision to pursue each of these three methods.
Methods We constructed a decision tree based on the presentation of a patient with suspected choledocholithiasis and an acceptable operative risk. The three choices modelled were preoperative ERCP with ES if CBD stones confirmed with stones extraction, LC/IOC with an additional decision if CBD stones found of intraoperative ERCP/ES or LCBDE with stone extraction (figure). The literature from 2010 to 2021 pertaining to these three methods were reviewed for data on duct clearance, morbidity, mortality, recurrence rate, length of stay (LOS), and operative time. The data for preoperative ERCP/ES was collected from 15 studies (n= 4935). For LCBDE the data was collected from 14 studies (n = 4376), whereas data for intraoperative ERCP/ES was collected from 7 studies (n = 1130).
Results The results are shown in the figure. Using the techniques over the last decade, preop ERCP/ES followed by LC had a duct clearance rate of 85.9%, a morbidity of 13.0%, mortality of 0.87%, a recurrent/retained stone rate of 7.3%, a LOS of 7.2 days, and an operative time of 118 minutes. LC/LCBDE had a duct clearance rate of 87.8%, a morbidity of 12.7%, mortality of 0.4%, a recurrent/retained stone rate of 1.98%, a LOS of 5.4 days, and an operative time of 122 minutes. LC with intraoperative ERCP/ES had a duct clearance rate of 98.14%, a morbidity of 8.5%, mortality of 0.2%, a LOS of 3.46 days, and an operative time of 116 minutes.
Conclusion Using data available from the last decade, LC with intraoperative ERCP/ES has the highest duct clearance, lowest morbidity and mortality, lower LOS, and a lower operative time. The caveat is that these data are based on the fewest studies published. Techniques, instruments, and training need improvement for LC/LCDBE to be a wider disseminated option.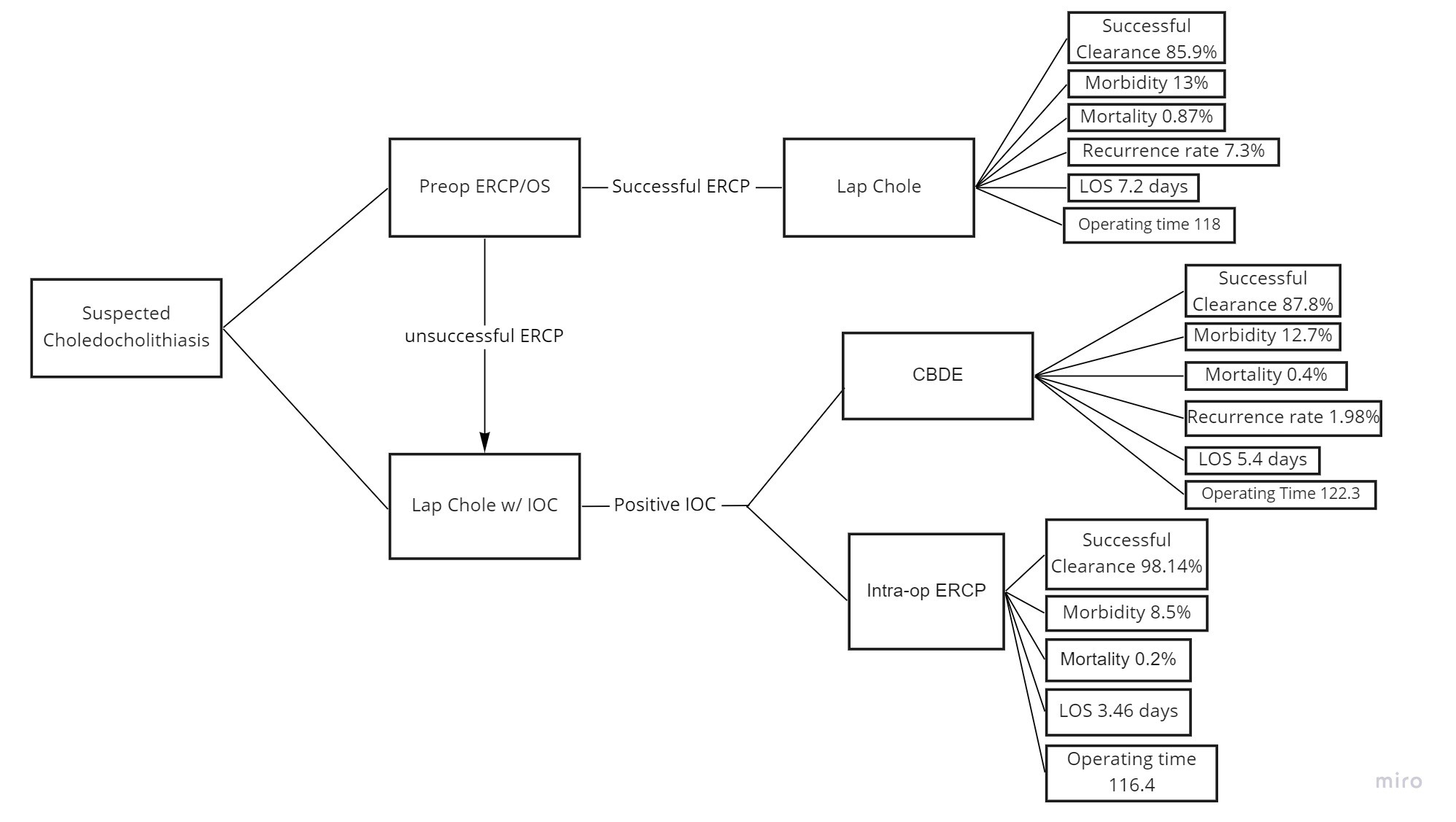
Back to 2022 Abstracts