
|
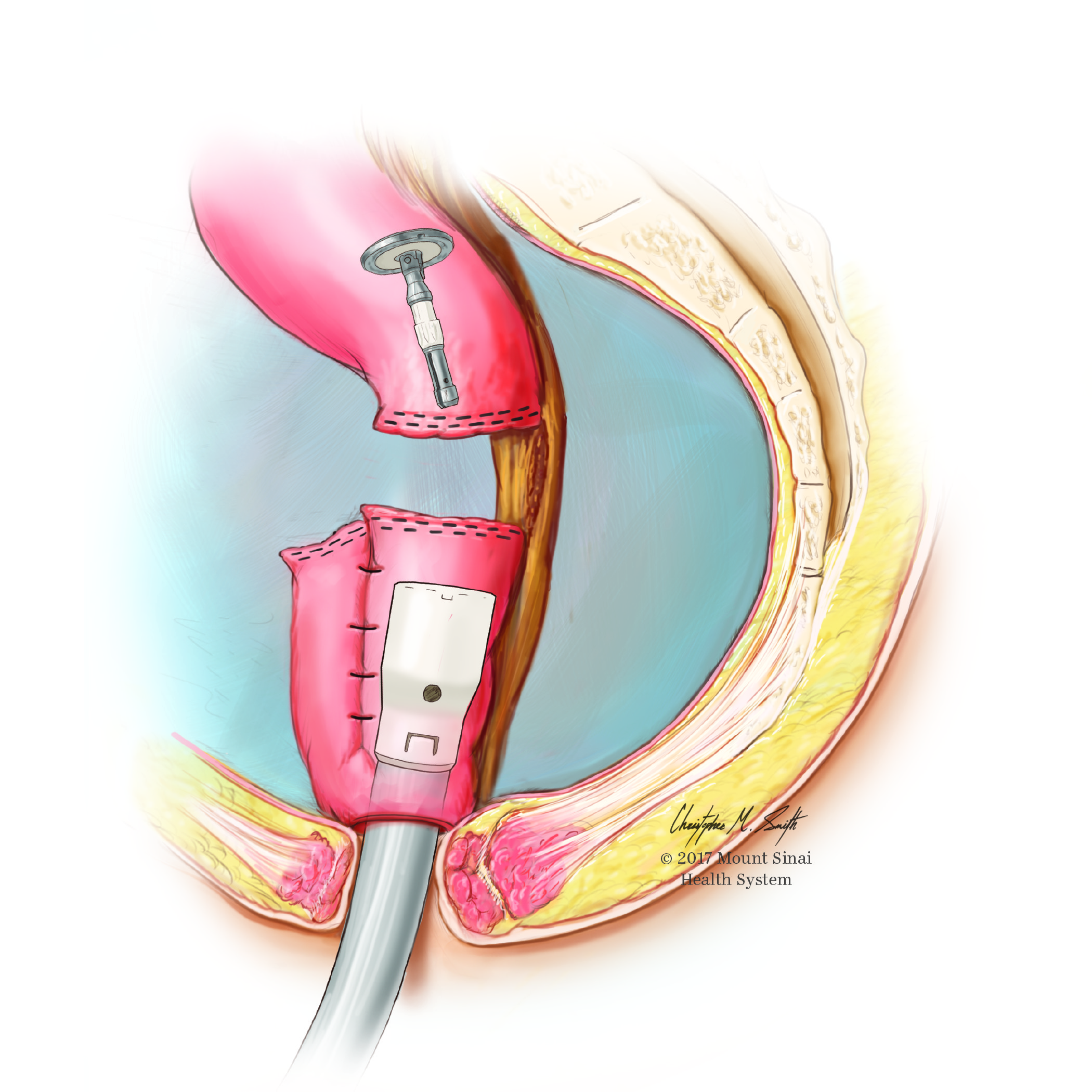
SURGICAL SOLUTIONS FOR INLET OBSTRUCTIONS IN J-POUCHES Brandon M. Elnekaveh*, Sue J. Hahn, Alexander Greenstein Surgery, Icahn School of Medicine at Mount Sinai, Great Neck, NY Background: Bowel obstructions can occur in up to 23% of patients after retorative procolectomy with ileal pouch-anal anastomosis (IPAA) for ulcerative colitis. Various mechanical changes including strictures or internal hernias can cause inlet obstructions after IPAA. They may be refractory to nonoperative or endoscopic management, and thus require surgery to bypass or resect the diseased bowel and salvage the patient's pouch. Methods: A retrospective review was performed of all patients of a single surgical practice who underwent a neo ileal-pouch anastomosis for J-pouch inlet obstructions between 2000 and 2017. Data collected included patient demographics, preoperative work-up, intraoperative findings, type of surgical intervention, and postoperative outcomes. Results: Surgical interventions were performed on 8 patients with J-pouch inlet obstructions. Six patients had inlet strictures or acute angulations at the inlet, which were either bypassed or resected and primarily anastomosed. Two patients had retromesenteric internal hernias, where their pouches volvulized posteriorly. Each underwent a partial pouch resection, neo ileal-pouch anastomosis and pouchpexy. Four of the five patients with inlet strictures were diagnosed with Crohn's disease. At a mean follow-up of 37 months, all patients were able to retain their pouches and the mean number of daily bowel movements was eight. There were two major operative complications. One patient had a fascial dehisence secondary to a deep organ space infection. She recovered well after a reexploration and primary closure. A second patient required a repeat partial pouch resection, neo-ileal pouch anastomosis and pouchpexy for a recurrent pouch volvulus. There were three minor complications. Discussion: J-pouch inlet obstructions may take years to develop, and can in some cases be due to the development of Crohn's disease at the pouch inlet. This study demonstrates that good functional results, including in patients with Crohn's disease, can be obtained with bypass procedures or partial pouch resection and neo ileal-pouch anastomosis in order to salvage a pouch and avoid pouch excision and permanent ileostomy. With increasing numbers of J-pouches being performed, novel surgical techniques are essential for maintaining patients' anorectal continence and quality of life. 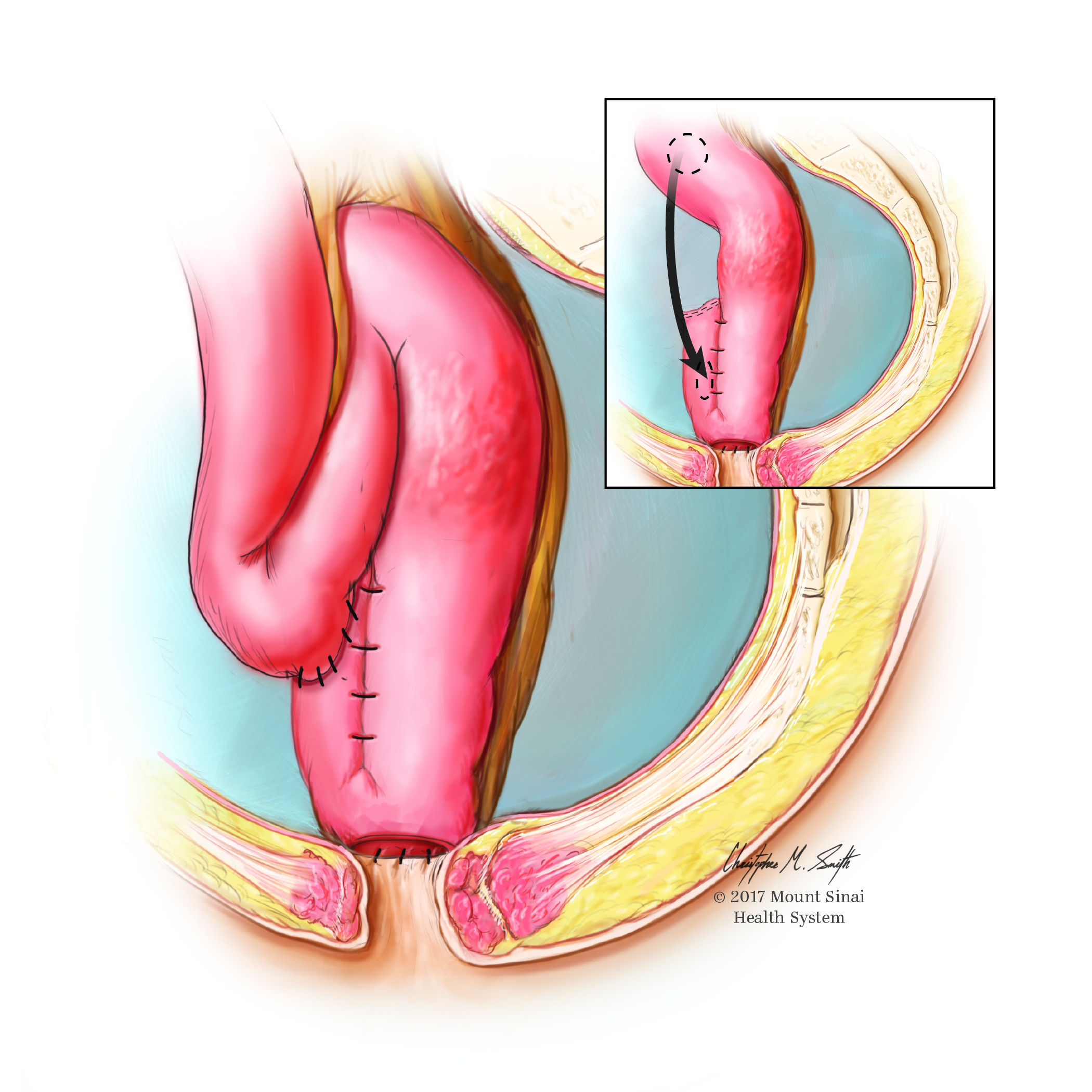
In-situ Bypass of Pouch Inlet Stricture Back to 2018 Posters |
|||||||||||||||
© 2026 Society for Surgery of the Alimentary Tract. All Rights Reserved. Read the Privacy Policy.