
|
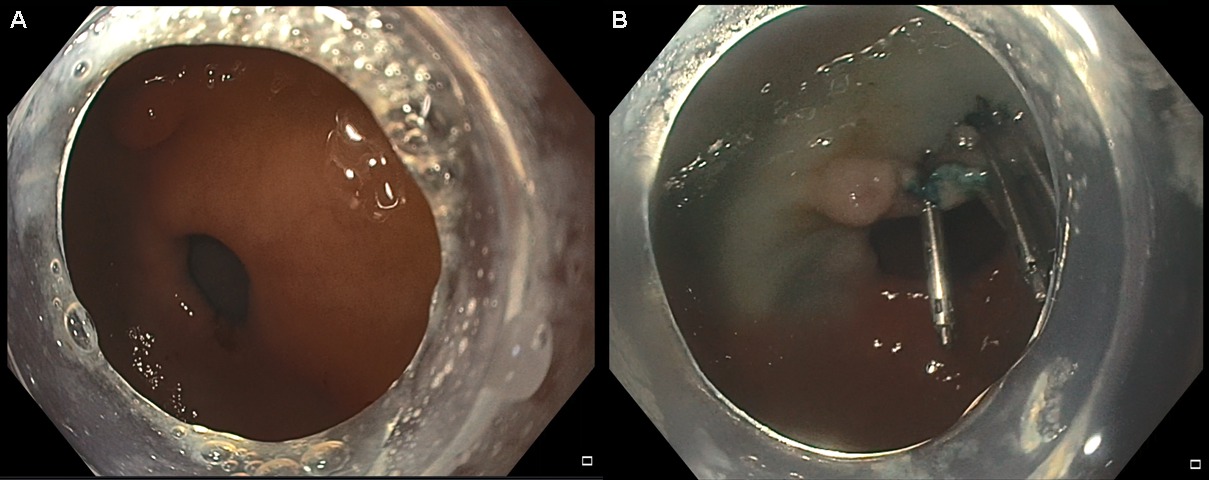
BEZOAR CLEARANCE PROTOCOL FOR ENDOSCOPIC PER-ORAL PYLOROMYOTOMY (POP): WHEN TO FIGHT ANOTHER DAY Marita D. Bauman*, Andrew T. Strong, John Rodriguez, Matthew Kroh, Jeffrey Ponsky, Matthew T. Allemang, Kevin M. El-Hayek General Surgery, Cleveland Clinic Foundation, Cleveland Heights, OH INTRODUCTION: Endoscopic division of the pylorus, per-oral pyloromyotomy (POP), is a promising new endoluminal therapy for medically refractory gastroparesis. While patients are instructed to follow a liquid diet for 4 days prior to scheduled POP procedures, significant solid food bezoars may still be encountered depending on disease severity. The presence of these bezoars preclude successful performance of the POP procedure and are often difficult to fully remove endoscopically. Herein, we detail a protocol developed at our institution to clear incidental bezoars prior to POP procedures. SUBJECTS and METHODS: Patients with severe medically-refractory gastroparesis, who at the time of initial attempted POP, were found to have gastric bezoars unable to be removed endoscopically were included. POP was first performed at our institution in January of 2016. A multimodal protocol for bezoar clearance was developed after a bezoar prevented safe performance of a POP. A large bore nasogastric (NG) tube (16-18 French) is inserted at the initial endoscopy and clamped. Patients are admitted to a regular nursing ward, kept nil per os (NPO), and the NG tube is flushed with 100 milliliters of normal saline every 4 hours. In addition, patients are medicated with a proton pump inhibitor, and scheduled intravenous metoclopramide (10mg every 6 hours) and intravenous erythromycin (250mg every 8 hours). The POP is then repeated the following day. RESULTS: Out of 147 POP procedures performed at our institution, 4 (2.7%) had incidentally noted bezoars that could not be cleared endoscopically, thus preventing safe performance of a POP (see Image 1). The four patients included 2 male and 2 female patients, with a mean age of 50.4 ± 8.3 years and mean body mass index of 30.8 kg/m2. Two had medically refractory diabetic gastroparesis, and two had medically refractory post-surgical gastroparesis. None were taking narcotics or pro-motility agents at the time the POP. The bezoar clearance protocol was successfully implemented in all 4 patients. On repeat upper endoscopy the following day, each patient had complete bezoar clearance (see Image 2). POP procedures were then completed, with an average procedure time of 22 minutes. All patients were discharged on post-POP day 1 (total length of stay 2 days), and there were no complications within 30 days of the procedure. CONCLUSIONS: The protocol for bezoar clearance prior to re-attempting POP has provided promising initial results, low patient risk, and without significant extended hospital stay. This protocol obviates the need for a prolonged endoscopy for bezoar clearance and allows POP to be performed in a safe operative field. 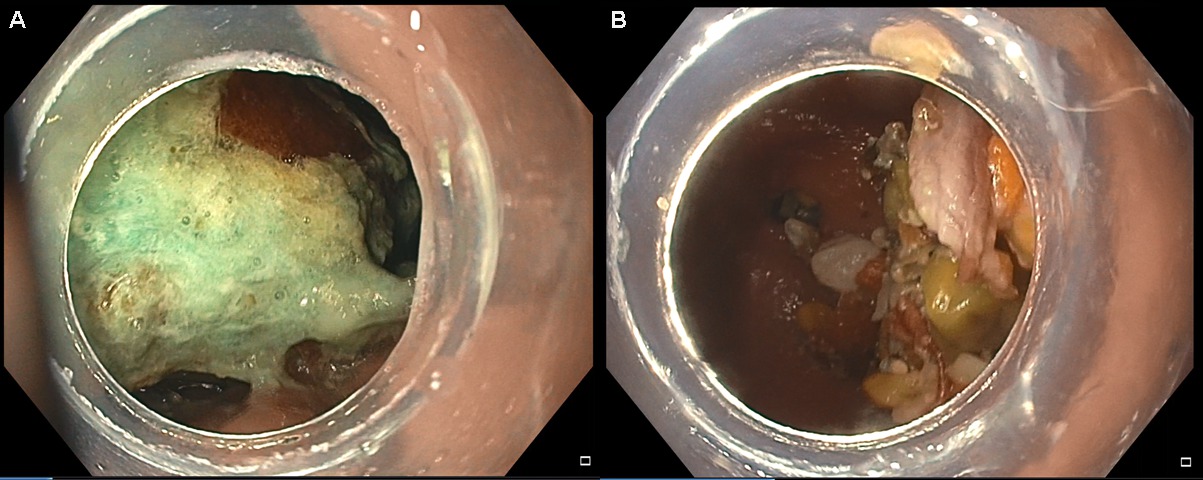
Image 1: Images of the intial endoscopy. (A) Immediately below the gastroesophageal junction. (B) Antrum and pylorus; food particles were actively refluxing through the pylorus. Back to 2018 Posters |
|||||||||||||||
© 2026 Society for Surgery of the Alimentary Tract. All Rights Reserved. Read the Privacy Policy.