|
Back to 2018 Posters
REDUNDANCY IN COLOGASTRIC ANASTOMOSIS FOLLOWING COLONIC ESOPHAGEAL REPLACEMENT FOR CORROSIVE UPPER GI STRICTURES
Kanagavel Manickavasagam1, Visvarath Varadarajan*2, Apsara Chandramohan3, Chandramohan Servarayan Murugesan1
1Dept of General, GI and Minimal Access Surgery, St Isabel Hospital, Chennai, India; 2Sri Ramachandra Medical College, Chennai, Tamilnadu, India; 3Govt Kilpauk Medical College, Chennai, Tamilnadu, India
BACKGROUND:
Colon is one of the preffered substitute for managing pharyngo-esophageal caustic strictures. The route of reconstruction is usually in the retrosternum or subcutaneous planes as esophagectomy is not done in most of the situations. It can be right colon, mid colon or the left colon and iso or anti peristaltic. Depending upon the distal transection site and cologastric anastomosis, there can be redundancy which may become clinically symptomatic, warranting revision.
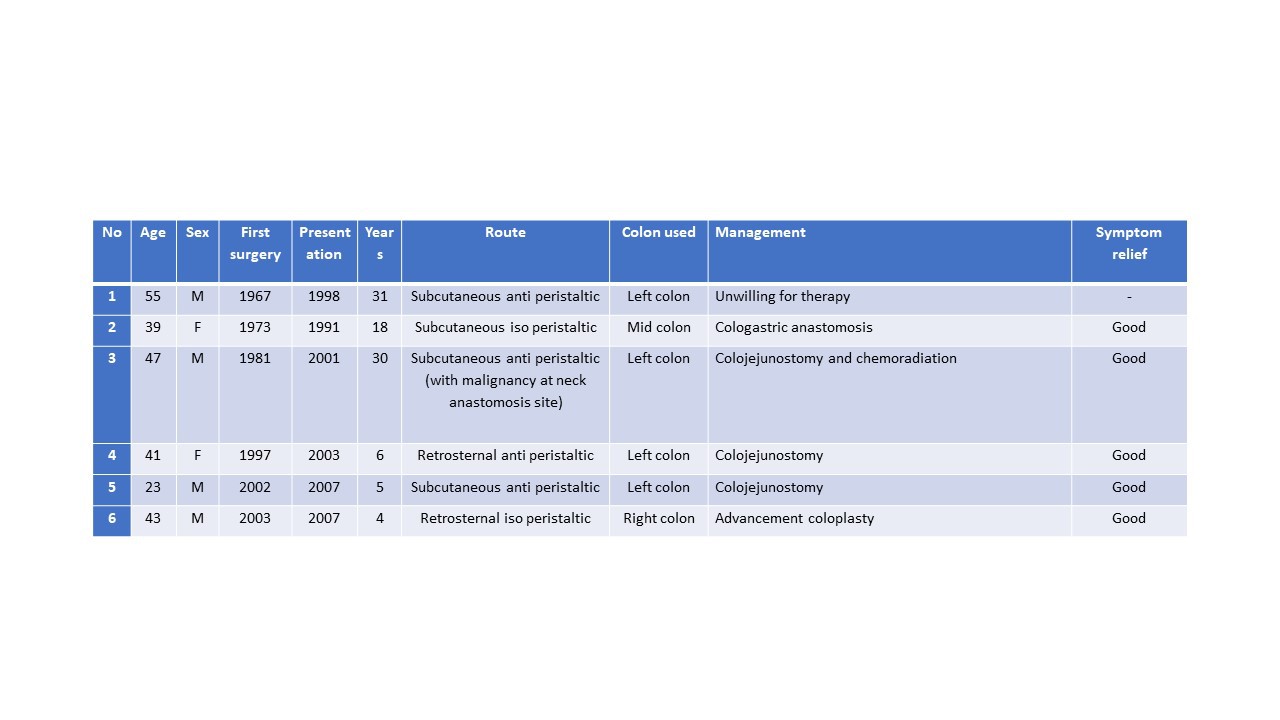
Methods: we have analysed our experience and management on 6 patients seen by us between 1991 and 2015..
Results: There was no mortality in this series of 6 patients. One patient was unwilling for treatment. Colojejunostomy was done for 2 patients, colojejunostomy with chemoradiation, revision cologastric anastomosis and advancement coloplasty were done for 1 patient each.
Discussion: Redundancy of cologastric anastomosis producing symptoms can present several years after primary reconstruction. Treatment has to be individualised.
Back to 2018 Posters
|
