
|
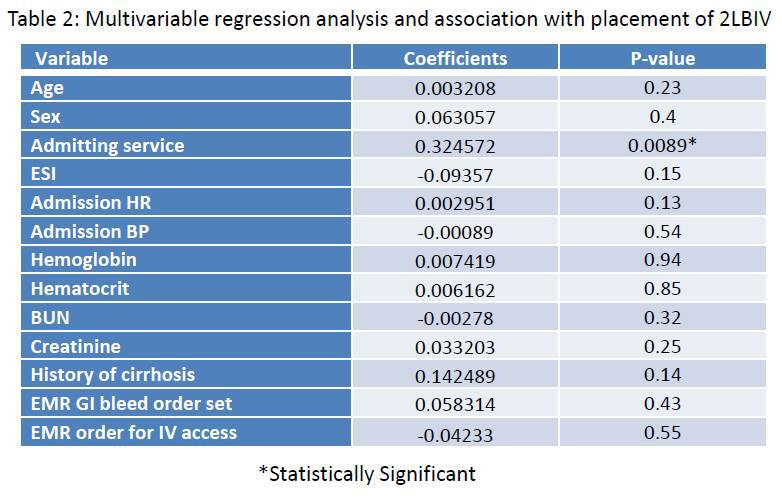
INTRAVENOUS ACCESS IN GASTROINTESTINAL BLEEDING: THE QUALITY GAP Andree Koop*, Neej Patel, Colt Cowdell, Lee Speicher Mayo Clinic Florida, Jacksonville, FL Background: Acute gastrointestinal bleeding (GIB) is common with substantial morbidity and healthcare costs. Current guidelines for the management of hospitalized patients with GIB recommend placement of two large bore intravenous lines (2LBIV), defined as an 18 gauge IV or larger. However, adherence to this recommendation is low and estimated to occur in less than 20% of patients. Methods: We conducted a retrospective study at a tertiary academic medical center of 100 consecutive patients who presented to the emergency department between January and May 2017 and required hospitalization for acute GIB. The study was performed as part of an internal medicine quality improvement project which utilized six sigma DMAIC methodologies to assess the quality gap in placement of IV access in patients hospitalized with GIB. We collected demographic, laboratory, and clinical data on hospitalized patients. The primary outcome was placement of 2LBIV in all patients admitted through the emergency department. Analysis was performed using a multivariable regression model. Results: Patient data are listed in table 1. Of 100 patients hospitalized with an admission diagnosis of GIB, only 14 patients had adequate IV access as defined by 2LBIV. In multivariable analysis, admission to the ICU was the only variable significantly associated with placement of 2LBIV (table 2). Notably, of patients with a history of cirrhosis, only 4/17 had 2LBIV. Thirty one of 100 patients were admitted with only a 20 gauge peripheral IV, and 27/100 patients had placement of 2 IVs although they did not meet criteria for 2LBIV. There was no association in multivariable analysis between 2LBIV and vital signs, laboratory values, the use of an order set specifically for GIB, or an order for placement of IV access within the electronic medical record. Discussion: This is the largest study evaluating IV access in patients hospitalized with GIB that we are aware of. Only 14% of patients had placement of 2LBIV in the Emergency department despite guideline recommendations. The only factor associated with 2LBIV was admission to the ICU, which is expected given the greater severity of illness in these patients. The effect of poor intravenous access on outcomes of hospitalized patients with GIB remains unknown. This data will be used to design a protocol for placement of 2LBIV in patients with GIB as part of a quality improvement initiative. 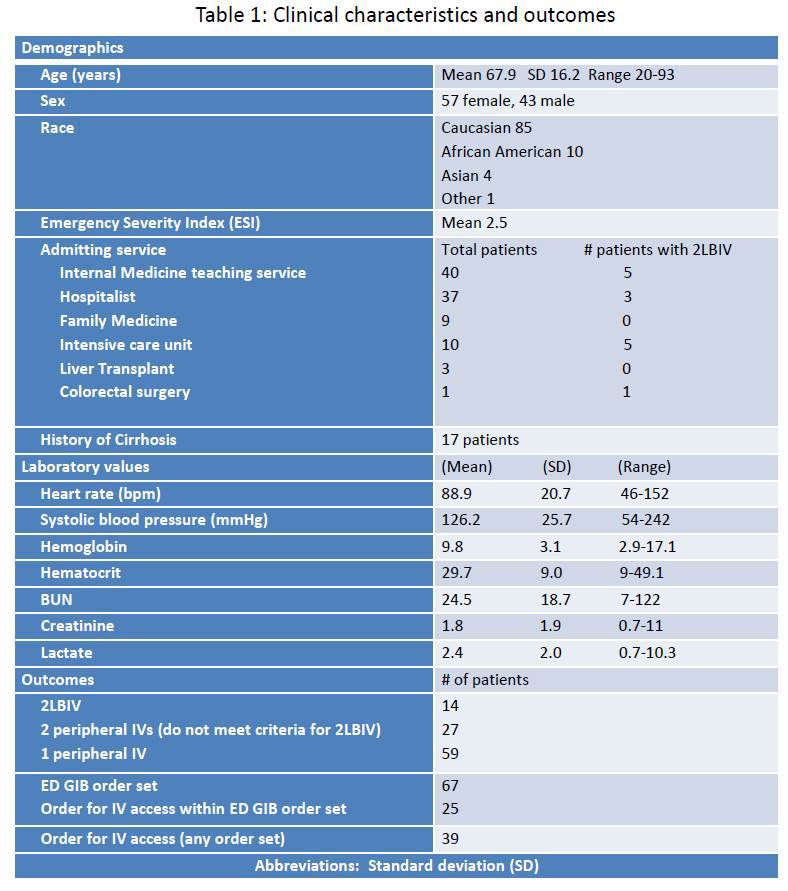
Back to 2018 Posters |
|||||||||||||||
© 2026 Society for Surgery of the Alimentary Tract. All Rights Reserved. Read the Privacy Policy.