
|
|
Back to 2017 Posters
LYMPH NODE RATIO IS AN IMPORTANT PREDICTOR OF OVERALL SURVIVAL INDEPENDENT OF GRADE AND STAGE IN PATIENTS WITH RESECTED GALLBLADDER CANCER
Darren S. Bryan*1, Mark S. Talamonti2, Nicholas R. Suss2, Andrew B. Schneider1, Andrew J. Benjamin1, Gaurav Ajmani2, Kevin K. Roggin1, David J. Bentrem3, Marshall S. Baker2
1Surgery, University of Chicago, Chicago, IL; 2Surgery, Northshore University Health System, Evanston, IL; 3Surgery, Northwestern University, Chicago, IL
Introduction
The value of formal lymph node assessment in the management of gallbladder cancer (GBAC) has not been well established. Previous studies have been limited by small sample sizes, variability in the number of nodes assessed, and heterogeneity of disease severity. We aim to identify factors associated with extent of lymphadenectomy, and determine the prognostic value of lymph node ratio (LNR) in gallbladder adenocarcinoma using a large nationally accruing dataset.
Methods
We queried the National Cancer database to identify patients undergoing surgical resection for GBAC between 2004 and 2013. Patients with metastatic disease, having R2 resections, or undergoing neoadjuvant treatment prior to resection were excluded from subsequent analysis. A subset analysis was then performed on patients undergoing what was considered to be an effort on the part of treating physicians to make a formal lymph node assessment. For this subset analysis patients with fewer than 3 examined lymph nodes were excluded.
Results
1,474 patients underwent resection for GBAC and met initial inclusion criteria. 264 patients underwent resection with lymphadenectomy involving assessment of ≥3 nodes. Multivariable regression controlling for age, facility type, comorbid conditions and pathologic stage identified treatment at academic research centers (HR 5.236 [2.649, 10.347]), integrated network cancer programs (HR 3.006 [1.385, 6.527]), and pathologic stage II (HR 1.596 [1.042, 2.442]), stage III (HR 3.564 [2.184, 5.815]) and IV disease (HR 4.607 [1.996, 10.634]) as independent predictors of a lymph node assessment including ≥3 nodes. On univariate analysis, overall survival varied inversely with lymph node ratio, with patients having LNR>0.2 demonstrating marked impairment in overall survival. 91 patients (34.5%) undergoing formal lymph node assessment had LNR>0.2. Multivariable Cox regression analysis controlling for age, comorbid conditions, facility type, surgical margin, tumor grade, and pathologic stage identified age >75 (HR 3.201 [1.601, 6.400]), pathologic stage III disease (HR 2.397 [1.208, 4.756]), LNR >0.2 (HR 1.651 [1.016, 2.684]) and receipt of adjuvant chemotherapy (HR 0.493 [0.278, 0.874]) to be independent predictors of overall survival.
Conclusion
Patients with GBAC are more likely to undergo a formal lymph node assessment if treated at academic or integrated cancer centers. Among GBAC patients with ≥3 nodes assessed, LNR >0.2 is a prognostic factor associated with decreased overall survival independent of pathologic stage and tumor grade and should be considered in decision making regarding adjuvant therapy.
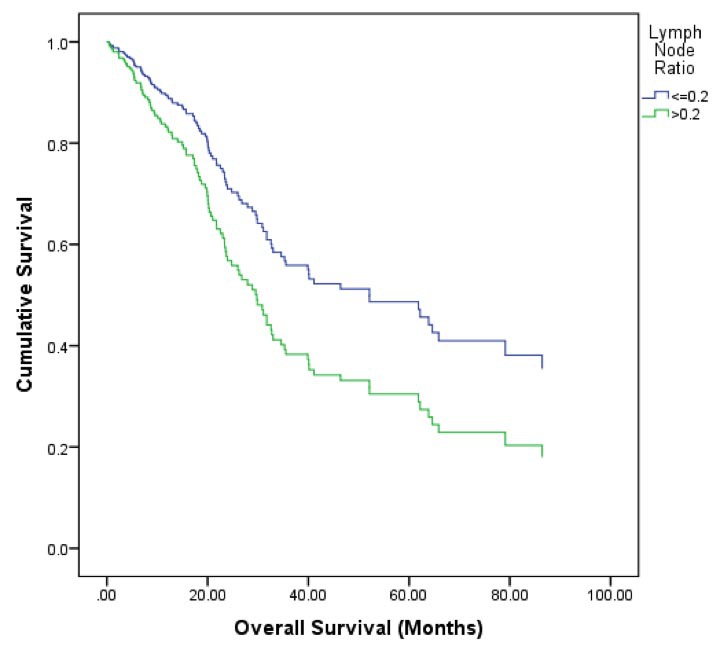
Figure 1: Cox proportional hazards modeling of Lymph Node Ratio in patients with gallbladder adenocarcinoma undergoing surgical resection with lymphadenectomy (≥3 nodes). Model adjusts for age, socioeconomic status, facility type, adjuvant treatment, pathologic stage, and grade
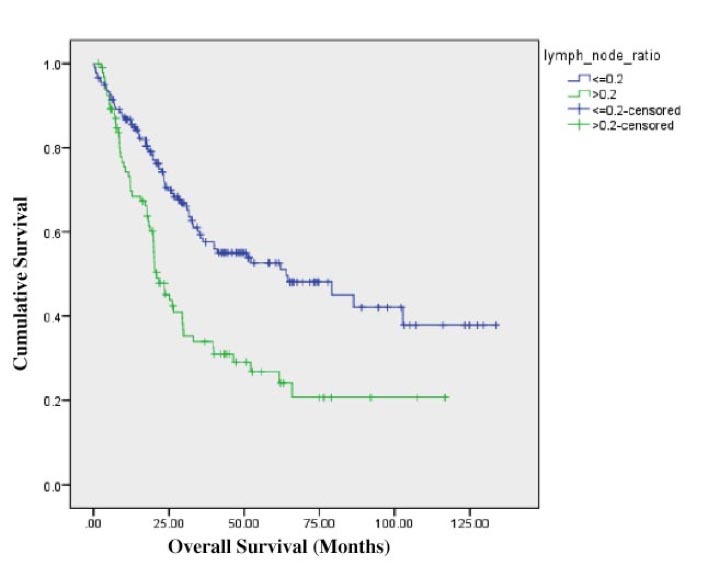
Figure 2: Kaplan-Meier estimator comparing LNR ≤0.2 with LNR >0.2.
Back to 2017 Posters
|

