|
Back to 2017 Posters
RECTAL CANCER IN PATIENTS UNDER 50 YEARS OF AGE
Anne M. Dinaux*1,2, Lieve G. Leijssen1,2, Hiroko Kunitake1,2, Liliana G. Bordeianou1,2, David L. Berger1,2
1General and Gastrointestinal Surgery, Massachusetts General Hospital, Boston, MA; 2Harvard Medical School, Boston, MA
Introduction
Population screening for colorectal cancer in the United States begins at the age 50. The incidence of colorectal cancer has steadily decreased in the population over 50 years of age; however, there has been a 1.8% increase in colorectal cancer rates per year in those younger than 50. This paper analyzes those patients who present with rectal cancer under the age of 50.
Methods
All patients who received surgical treatment for their primary rectal cancer between 2004 and 2015 at a single center were included, with exclusion of those without preoperative staging imaging. Patients were retrieved from a retrospective, prospectively maintained, IRB approved database. The cohort was divided based on age under or over 50 years to compare differences in short term outcomes, as well as oncological long-term outcomes.
Results
A total of 623 patients were included; 136 patients under and 487 patients over 50 years of age. ASA-score was significantly higher in the older group (mean 2.31 vs. 2.06; P<0.001), BMI did not differ between the two groups and 22% of the older patients were diagnosed through screening compared to only 5.1% of the younger patients (P<0.001).
Clinical staging differed significantly mainly due to significantly more Stage IV patients in the younger group. The rates of clinically locally advanced disease (excluding patients with clinically Stage IV disease) were comparable between the 2 groups (65.1% in young patients vs. 68.2% in older patients; P=0.540). Neoadjuvant treatment rates showed no significant differences. In line with clinical staging, pathologic AJCC staging differed mainly due to a higher baseline metastasis rate in the younger group (22.8% vs. 12.1%; P=0.002). Pathologic characteristics showed no significant differences. Operative duration was comparable, while admission duration was significantly shorter in the younger patients (medians: 4 vs. 5 days; P=0.011). Adjuvant treatment rates were also higher in the younger patient group (69.9% vs. 54.6%; P=0.001), and as a result of the higher baseline metastasis, the rectal cancer death rate was 15.4% in the young patient group, compared to 9.2% in the older group (P=0.038). Stage for stage comparison showed no significant differences between the two age groups in long-term outcomes nor in survival curves (fig. 1 & fig. 2).
Conclusions
Rectal cancer patients younger than 50 do not have more aggressive disease; rather they present with more advanced disease. When assessing oncological long-term outcomes in a stage for stage fashion, there is no difference between those patients who present when they are younger than 50 years of age and those who are older. It might be reasonable to conclude that the lack of screening colonoscopy in those younger than 50 leads to the difference in stage at presentation.
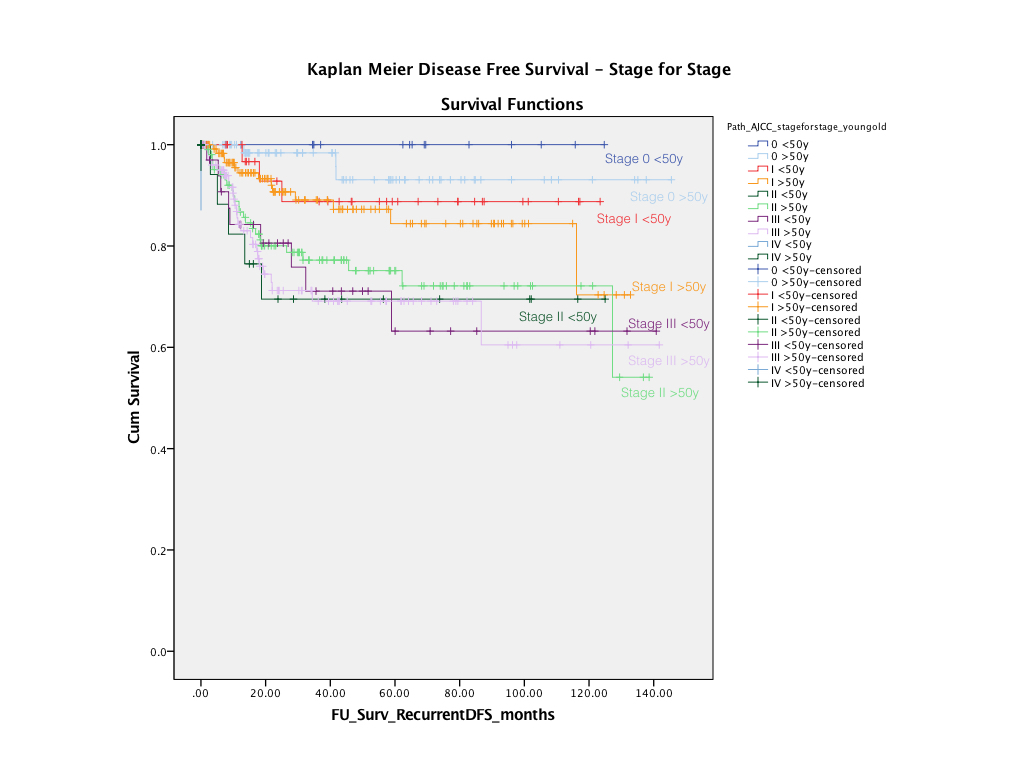
Fig. 1 Kaplan Meier Recurrent disease free survival
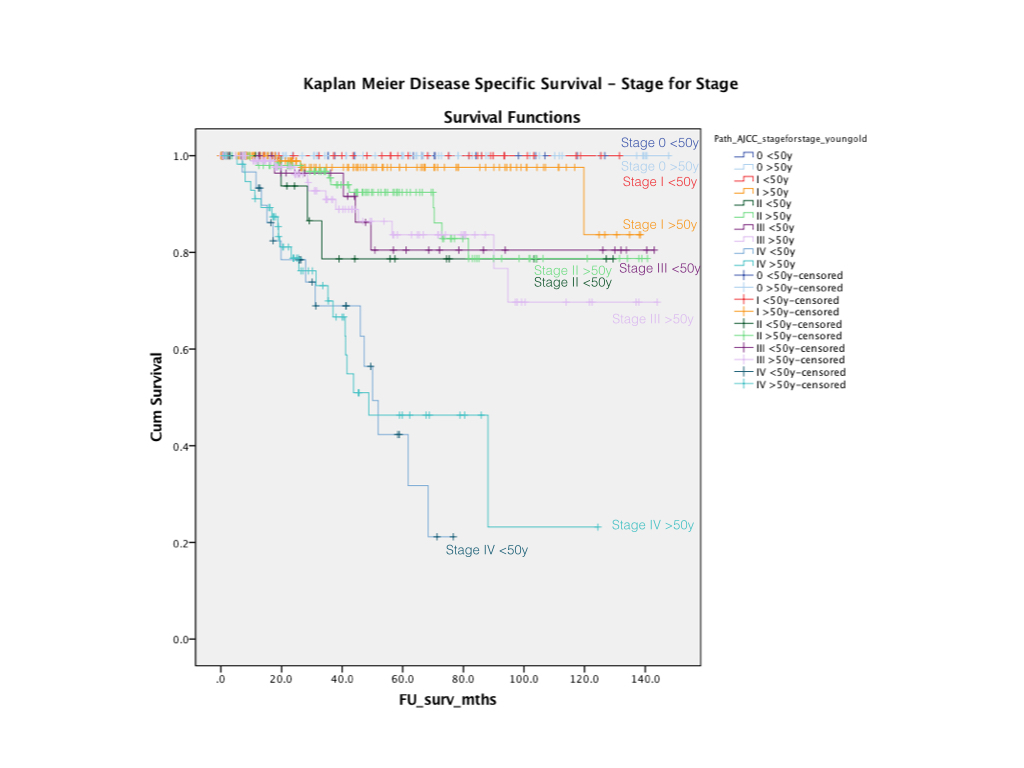
Fig. 2 Kaplan Meier Disease specific survival
Back to 2017 Posters
|

