|
Back to 2017 Posters
30-DAYS ARE INADEQUATE FOR ASSESSING READMISSION FOLLOWING COMPLEX HEPATOPANCREATOBILIARY PROCEDURES
Maria Altieri*, Jie Yang, Donglei Yin, Konstantinos Spaniolas, Mark A. Talamini, Aurora D. Pryor
General Surgery, Stony Brook University Hospital, Stony Brook, NY
Introduction:
Early readmissions (30-days) have been used as a measure of health care quality. However, many are questioning if the 30-days period is enough, especially for complex, high-morbidity hepatopancreatobiliary (HPB) procedures. The purpose of our study was to evaluate patterns of readmission for a longer period (up to 2 years) following HPB surgery in the state of New York (NY).
Methods:
Following Institutional Review Board (IRB) and NY Department of Health (DOH) approvals, the State Planning and Research Cooperative System (SPARCS) administrative database was utilized. Through the use of ICD-9 procedure codes, we identified patients undergoing complex HPB procedures between 2010-2012. Patients were followed for two years following surgery to identify all-cause re-admissions. Factors studied for post-operative hospital admission included patient demographics, presence of co-morbid conditions, procedure type, and academic versus non-academic status of a hospital. 30-day admission was also checked if it predicted long-term readmissions. Univariate generalized linear mixed models (GLMM) were used to estimate marginal associations between outcomes. Univariate logistic regression with firth bias correction were used when GLMM had convergence issues. Statistical analysis was performed using SAS 9.4 and significance level was set at 0.05.
Results:
Between 2010-2012, 4,147 complex HPB procedures were identified. From these, there were 779 (18.78%) unplanned 30-day readmissions, 1326 (31.97%) unplanned 30-day to 1 year readmissions, and 906 (21.85%) 1-2 year readmissions. Risk factors for 30-day readmissions include facility type, as academic centers are more likely to have a readmission (OR 1.5, 95% CI 1.13-2), presence of any co-morbidity (OR 1.6, 95% CI 1.3-2.1) and post-operative complications (OR 1.4, 95% CI 1.2-1.6). Risk factors for one-year readmission include male gender (OR 1.2, 95% CI1.1-1.4), race, any co-morbidity (OR 1.96, 95% CI 1.56-2.46) or any post-operative complication (OR 1.19, 95% CI 1.03-1.36), and 30-day readmission (OR 2.13, 95%CI 1.81-2.51). Risk factors for up to 2 year readmissions included male gender (OR 1.16, 95% CI 1.0-1.35), presence of any co-morbidity (OR 1.33, 95% CI 1.05-1.68), and previous 1-year readmission (OR 2.14 95% 1.83-2.5). Top 5 ranked Reasons for readmissions are displayed in Table 1.
Conclusion:
The 30-day readmission window is an inadequate, but predictive, measure of total readmission following complex HPB procedures. Complications and prevision readmission are significant reasons for readmission up to 2 years following complex HPB procedures.
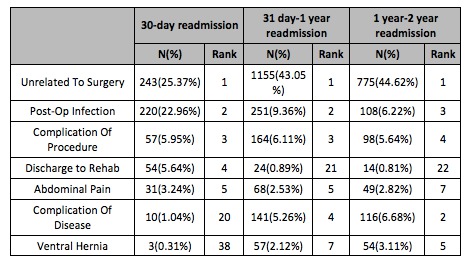
Table 1. Reasons for readmission following complex hepatopancreatobiliary procedures.
Back to 2017 Posters
|

