|
Back to 2017 Posters
ERAS IN THE COMMUNITY HOSPITAL: STEPWISE APPROACH TO QUALITY IMPROVEMENT
Shane M. Svoboda*1, Daniel Galante1, Joann Coleman1, Karen Sweeney1, David Blumberg1, Vanita Ahuja1,2
1Surgery, Sinai Hospital, Baltimore, MD; 2Sidney Kimmel Medical College, Philadelphia, PA
Introduction: Enhanced recovery after surgery (ERAS) programs have been successful in many academic centers; however, their efficacy in a community hospital remains unclear. A community hospital in Maryland implemented the ERAS protocol for elective colorectal (CR) surgery in January 2015. We hypothesized that a resident-led quality improvement project with a multi-disciplinary team stepwise approach can be established at a community hospital to implement ERAS successfully. Our aim was to reduce hospital length of stay and surgical site infections (SSI).
Method: Baseline data from the American College of Surgeon (ACS)- National Surgical Quality Improvement Program (NSQIP) was used to establish and monitor 30-days postoperative outcomes. A nursing team was educated on ERAS protocol and adherence to each measure. The project was accomplished in 18 months with a bundled approached implemented every six-months. Positive outcomes were initially observed in a limited number of measures. The goal was to continue with the protocol to realize improvement in all measures of the protocol in a stepwise approach to enhance patient outcomes. Continuous monitoring and systematic timely communication of the results were measured and communicated to encourage staff to sustain behavior changes.
Results: Data was collected on a total of 215 patients over the time period with mean age of 65 years (105 males, 110 females). In the first six months, educational materials were developed and information was disseminated to patients, key stakeholders, and medical staff. ACS-NSQIP data for the base time period (CY2014) when compared to national average was higher for LOS ( 9.5 days vs. 8.7 days) while below for SSI (5.7% vs. 10.8%). The second step was rolled out for the next months with implementation of each measure. The third step was Jan-June 2016 with assessment of compliance of each measure in partnership with nursing. The final data was assessed in August 2016 which showed that our LOS decreased by 15% compared to Jan 2015 (Table 1); while SSI rate increased by 4.6% (Table 2). A quick assessment showed that we had not educated our new surgeons on our wound barrier for SSI prevention. The next step is to educate all staff and reintroduce a CR wound infection bundle to decrease SSI rate.
Conclusion: Concurrent data from ACS-NSQIP can be used to assess performance evaluation and to identify the determinants of outcomes achieved at a community hospital. A stepwise approach can be a successful strategy to implement a complex protocol at a community hospital with reduced resources. This approach helped us to bundle our resources, engage our team to sustain quality improvement while continuing to focus on improving the next quality measure.
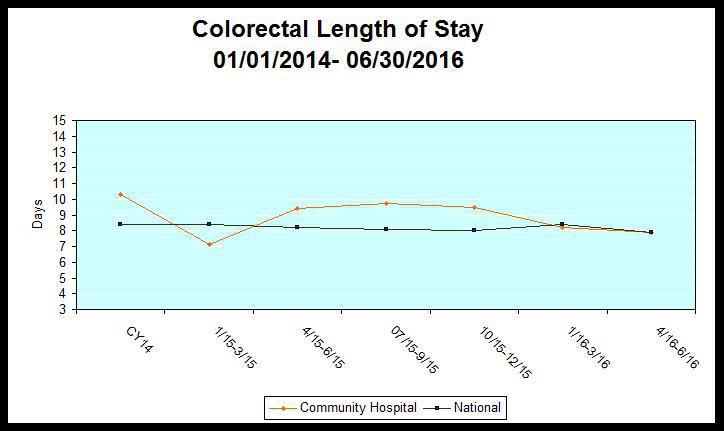
Table 1: Length of Stay in Colorectal Surgery Patients
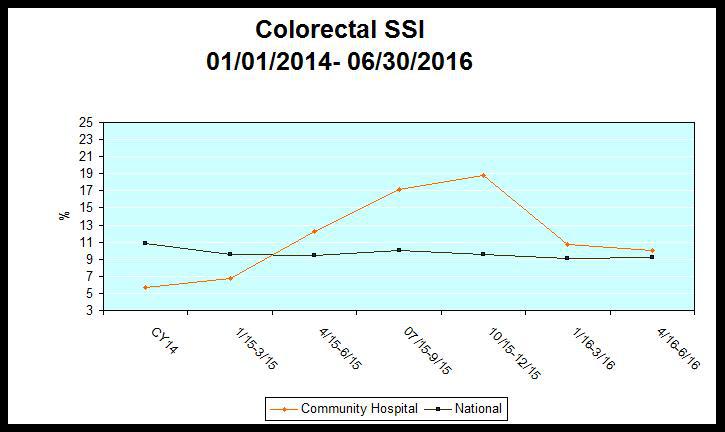
Table 2: Surgical SIte Infection in Colorectal Surgery Patients
Back to 2017 Posters
|

