|


|
Back to 2017 Program and Abstracts COMBINED EMR AND EXTENDED LAPAROSCOPIC APPENDECTOMY FOR THE TREATMENT OF CECAL ADENOMAS INVOLVING THE APPENDICEAL ORIFICE: A NOVEL TECHNIQUE Emily Huang*1, Ahmed S. Alkoraishi2, Craig A. Munroe3 1Surgery, UCSF, San Francisco, CA; 2Surgery, Kaiser San Francisco, San Francisco, CA; 3Gastroenterology, Kaiser San Francisco, San Francisco, CA
Introduction: Surgical resection is the gold standard in treatment of neoplasia involving the appendiceal orifice (AO). Endoscopic mucosal resection (EMR) of adenomas involving the AO can be challenging for several reasons: 1) resection into the AO carries a risk of appendicitis; 2) the lack of muscularis propria at the os increases the risk of perforation; and 3) it is difficult to guarantee a negative deep margin for polyps growing into the lumen of the appendix. Alternatively, surgical cecectomy for primary resection of AO lesions is limited by the difficulty of ensuring a negative lateral margin without compromising the ileocecal valve; this usually necessitates an ileocecal resection with anastomosis. Although there are reports of EMR for the management of polyps involving the AO, and combined endoscopic and laparoscopic surgery (CELS) has become more widely accepted for a variety of conditions, a structured and combined approach to lesions involving the AO has yet to be described. We describe a novel approach to the treatment of cecal tumors involving the AO—and present an algorithm to guide decision-making regarding when these techniques should be applied.
TA = tubular adenoma TVA = tubulovillous adenoma VA = villous adenoma SSA = sessile serated adenoma IC = intramucosal carcinoma 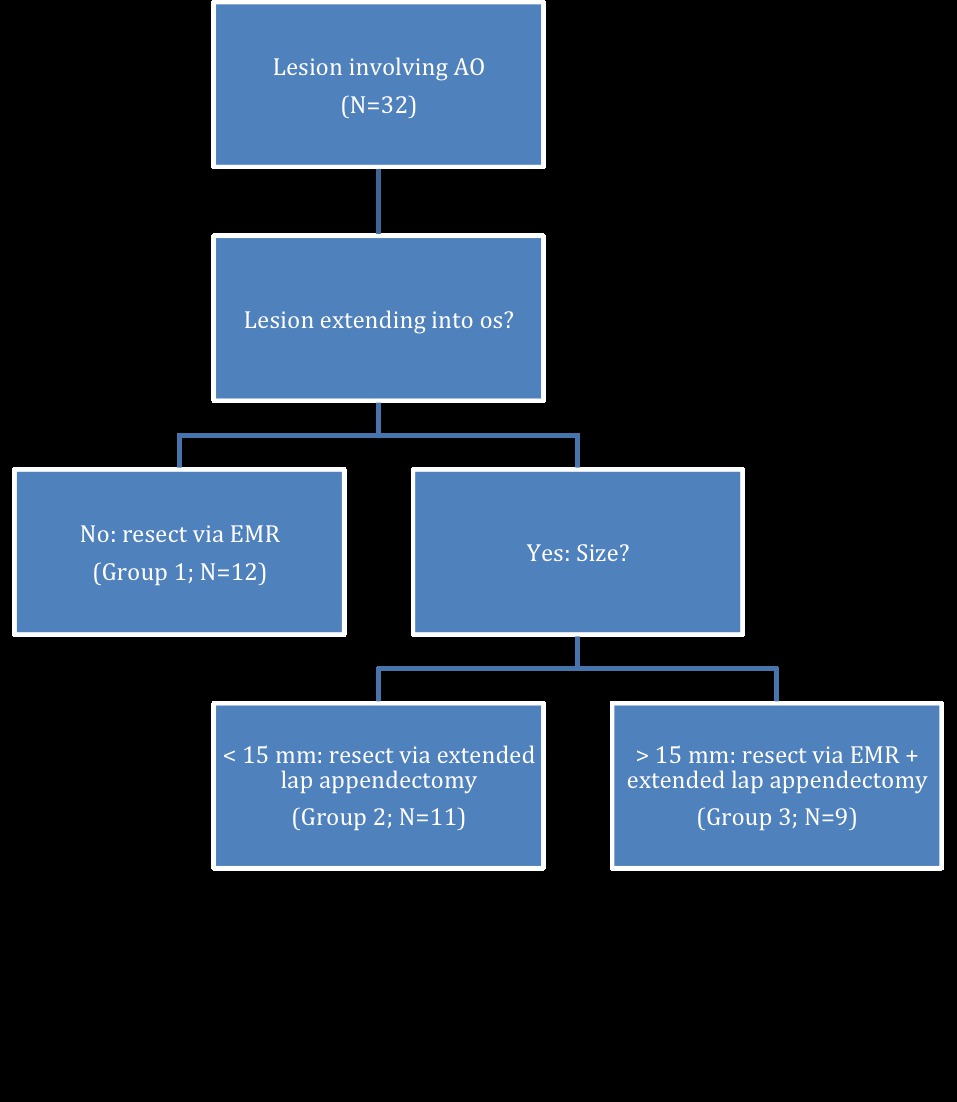 Figure 1: Decision algorithm for the use of EMR and extended laparoscopic appendectomy in treating cecal adenomas involving the appendiceal orifice Back to 2017 Program and Abstracts |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
© 2026 Society for Surgery of the Alimentary Tract. All Rights Reserved. Read the Privacy Policy.