|
Back to 2017 Program and Abstracts
COMPLETE LATERAL LYMPH NODE DISSECTION USING A TRANSABDOMINAL AND EXTRAPERITONEAL APPROACH: AVOIDING LOCAL RECURRENCE IN LOW RECTAL CANCER
Akira Ouchi*, Koji Komori, Takashi Kinoshita, Taihei Oshiro, Yasuhiro Shimizu
Department of Gastroenterological Surgery, Aichi Cancer Center Hospital, Nagoya, Aichi, Japan
Objective: Mesorectal excision (ME) with autonomic nerve-preserving lateral lymph node dissection (ANP-LLND) is a standard procedure for low rectal cancer in Japan. However, complete lymph node dissection of the obturator and internal iliac region is difficult because of the narrow field of vision in the pelvic cavity. Our ANP-LLND using a transabdominal and extraperitoneal approach provides a wider field of vision through the paravesical space and enables us to perform complete lymph node dissection of these regions. Here we introduce our ANP-LLND procedure and report the clinical and oncological outcomes.
Methods: After ME, hypogastric nerves were separated and secured to be preserved. First, common iliac nodes were dissected; presacral nodes were also dissected by exposing the pelvic surface of the sacrum through a transabdominal approach. Internal iliac nodes to superior vesical artery were dissected; furthermore, external iliac nodes were dissected toward the inguinal ligament farthest from the abdominal side. Then, the paravesical space was opened via an extraperitoneal approach, and obturator nodes were observed through the paravesical space and were completely dissected while preserving the obturator nerve, resecting the obturator artery and vein, and confirming lateral pelvic wall and sciatic nerve. External iliac nodes were also dissected from the inguinal ligament. Finally, internal pudendal nodes from the coccygeal muscle were completely dissected while preserving the superior vesical artery and the pelvic plexus, and transecting several inferior vesical arteries.
Results: Between 2007 and 2016, we performed ME with ANP-LLND for 225 patients with cT2 or deeper low rectal cancer. The median operative time was 371 min, and the median blood loss was 610 ml. Postoperative complications developed in 112 (49.7%) patients, and the most frequent one was pelvic cavity infection in 39 (17.3%) patients. Temporary urination disorder developed in only 15 (6.6%) patients, and persistent urination disorder required intermittent urethral catheterization developed in only one woman. Lymph node metastasis was pathologically found in 64 (28.4%) patients after LLND. Local recurrence-free survival in all patients and those with pT3 or deeper low rectal cancer at 5 years was 88.9% and 84.3%, respectively. Overall survival in all patients and those with pT3 or deeper low rectal cancer at 5 years was 86.0% and 81.9%, respectively.
Conclusions: Our ANP-LLND provides a wider field of vision in the pelvic cavity through the paravesical space via an extraperitoneal approach, and results in favorable clinical and oncological outcomes.
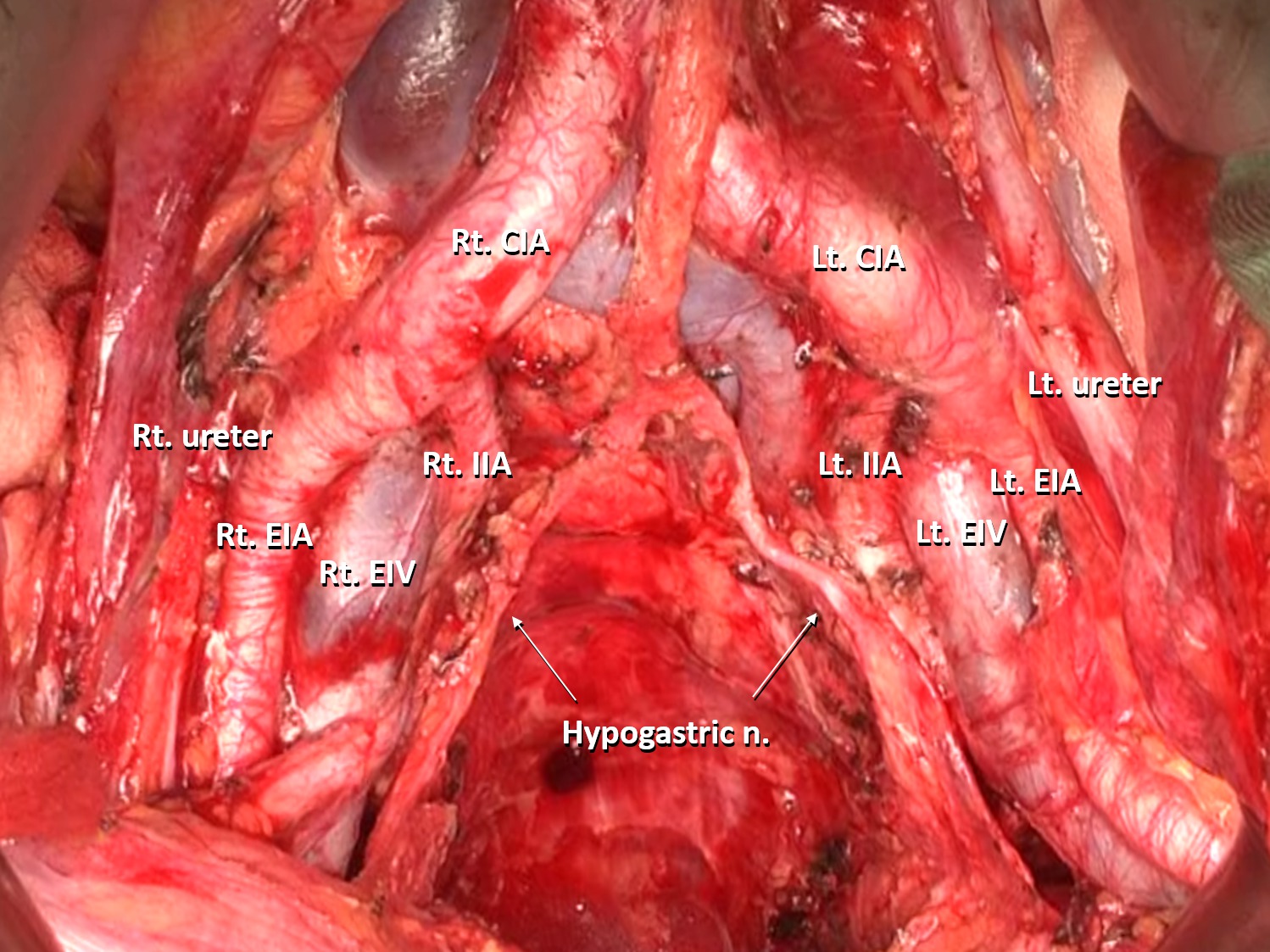
A transabdominal view of the pelvic cavity after mesorectal excision with autonomic nerve-preserving lateral lymph node dissection
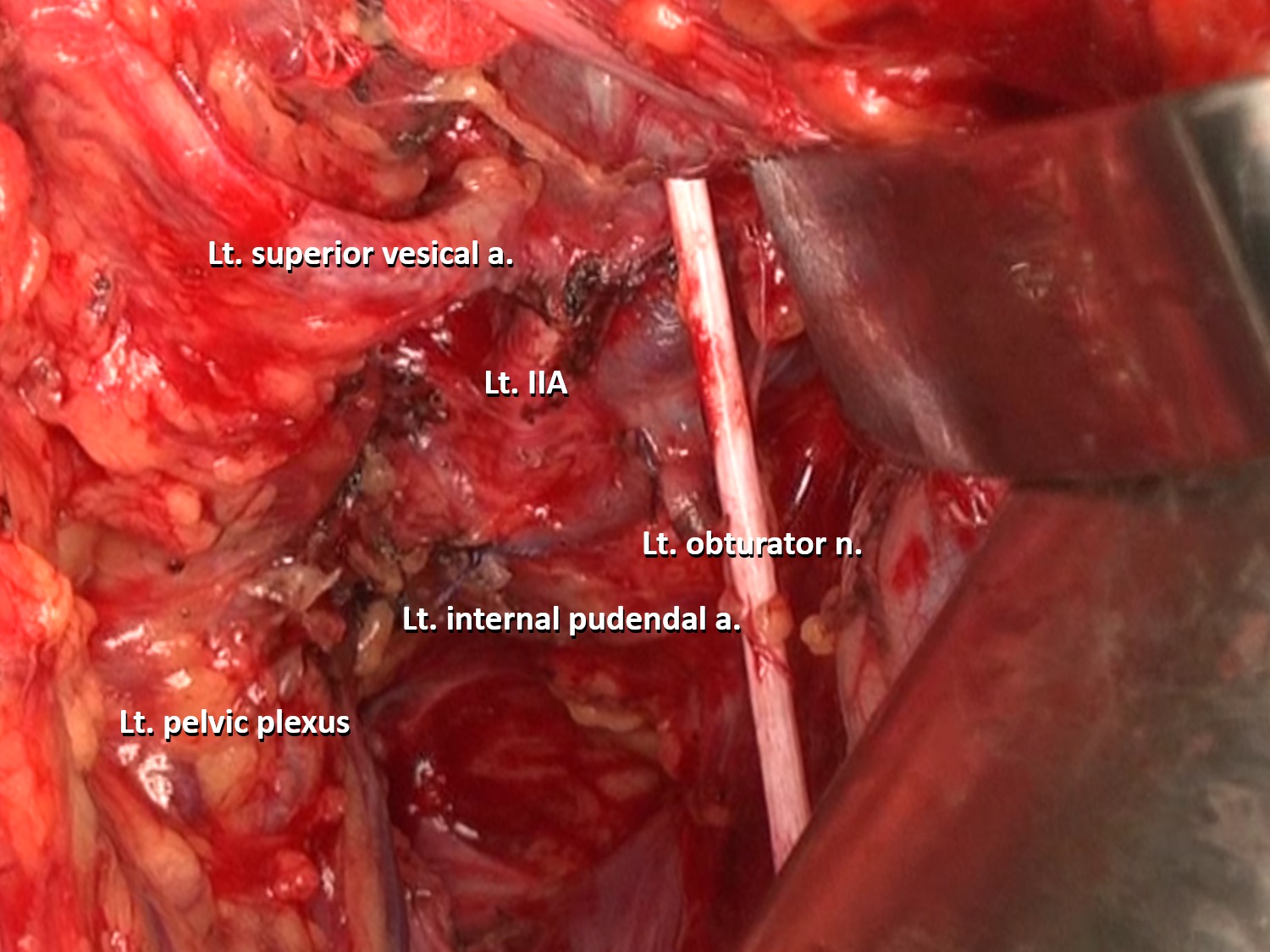
An extraperitoneal view of the paravesical space after mesorectal excision with autonomic nerve-preserving lateral lymph node dissection
Back to 2017 Program and Abstracts
|

