|
Back to 2017 Program and Abstracts
RE-RESECTION OF A POSITIVE PANCREATIC MARGIN IS ASSOCIATED WITH PROLONGED SURVIVAL AMONG PATIENTS WITH PANCREATIC CANCER TREATED WITH PREOPERATIVE THERAPY AND PANCREATODUODENECTOMY
Michael E. Egger*, Laura R. Prakash, Jordan M. Cloyd, Huamin Wang, Michael P. Kim, Ching-Wei Tzeng, Thomas Aloia, Jean Nicolas Vauthey, Jason B. Fleming, Jeffrey E. Lee, Matthew Katz
Surgical Oncology, University of Texas MD Anderson Cancer Center, Houston, TX
Introduction: The role of re-resection of a positive pancreatic transection margin on the basis of intraoperative assessment in patients undergoing de novo pancreatoduodenectomy for cancer has recently been debated. Preoperative therapy may improve margin-negative resection rates and select patients with “favorable tumor biology” for surgery. We therefore hypothesized that re-resection of a positive pancreatic transection margin to a negative one prolongs survival following preoperative therapy.
Methods: The records of consecutive patients who underwent pancreatoduodenectomy following the administration of chemotherapy and/or chemoradiation between 2000-2014 at a single center were reviewed. The intraoperative assessment of each patient’s pancreatic margin was compared to its final status, which was categorized as negative, converted by re-resection to negative, or positive. The superior mesenteric artery (SMA) margin was defined as negative if ≥ 1mm. Kaplan-Meier survival analysis and multivariable Cox proportional hazard modeling was performed for overall survival (OS) and recurrence-free survival (RFS).
Results: A positive pancreatic transection margin was identified intraoperatively in 52 (11%) of 471 patients. The final pancreatic margin was reported as negative in 415 (88%), converted by re-resection to negative in 39 (8%), and positive in 17 (4%) patients. 28 (72%) patients in whom the pancreatic margin was converted from positive to negative had a negative SMA margin and 18 (46%) had negative lymph nodes. Patients in whom the pancreatic margin was converted to negative had a longer OS than those in whom the final margin was positive, even after controlling for other factors (multivariable HR 0.48, 95%CI 0.24-0.97; Figure). However, conversion was not associated with a prolongation of RFS (multivariable HR 0.67, 95% CI 0.30-1.27). The five year OS rate was 24% in the converted margin group and 31% in the negative margin group; there were no five year survivors in the positive margin group.
Conclusion: In patients with pancreatic cancer treated with preoperative therapy and pancreatoduodenectomy, the status of the pancreatic transection margin should be determined intraoperatively, and re-resection of a positive margin should be performed when technically feasible.
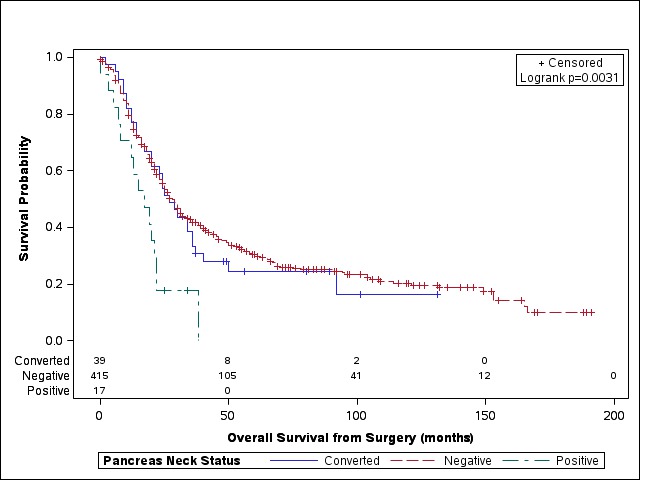
Figure. Overall survival from pancreatoduodenectomy for pancreatic ductal adenocarcinoma following neoadjuvant therapy, stratified by the pancreas neck margin status.
Back to 2017 Program and Abstracts
|

