|
Back to 2015 Annual Meeting Program
Isolated Corrosive Gastric Strictures - New Working Classification and Management Strategies
Kanagavel Manickavasagam*1, Asmita Chandramohan2, Kannan Devigounder2, Chandramohan Servarayan Murugesan2
1Dept of General, GI and Minimal Access Surgery, St Isabel Hospital, Chennai, India; 2Institute of Surgical Gastroenterology, Madras Medical College, Chennai, India
Corrosive injuries to the upper gastrointestinal tract is one of the difficult problems to treat. It resultsin major morbidity and mortality. Corrosives are substances which corrode and destroy tissues through direct chemical reaction. The strictures can present with various severity in pharynx, oesophagus and stomach. Isolated gastric strictures are less observed. Although corrosive substances can reach rapidly from oesophagus onto the stomach, they get stagnant in the prepyloric region because of pyloric spasm. The stricture may involve antrum, body and the pyloroduodenal area or diffusely the entire stomach depending upon the rapidity of spread of the ingested corrosive substance.
We have classified the gastric strictures so as to optimize the treatment options based on the subtype. We herewith formulate a new working classification. Treatment options according to the classified subtypes are also suggested to optimize the outcome.
Data: 48 patients of isolated gastric stricture were included in this study. We had 20 patients with Type I; 12 underwent arcade preserving antrectomy, 14 had Bilroth Type I and 6 had Bilroth Type II restoration. We had one Type IIA; managed by strictureplasty. Four Type IIB; managed with pylorus preserving antrectomy. We had three Type III; treated by circumferential sleeve resection and gastrogastrostomy. We had five Type IV; managed with total gastrectomy. We had one Type V; managed by limited oesophagogastrectomy. We had three Type VI; managed by gastrojejunostomy as these patients had first part duodenal involvement. We had eleven Type VII; called as gastrocele; managed with antrectomy and colon pullup in five, gastrojejunostomy and colon pullup in three and antrectomy and retrograde dilatation in two. One patient died due to massive aspiration prior to treatment. There were acceptable morbidiy and two mortality in this series. Our new working formulation will form the basis of care in patients with gastric corrosive strictures.
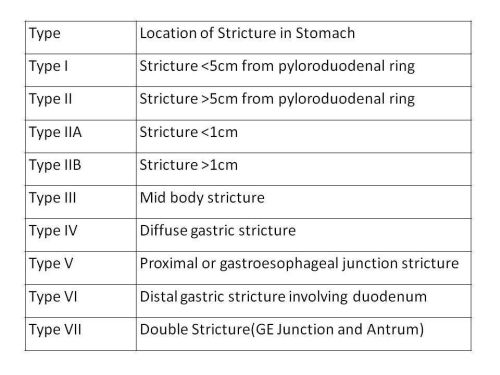
NEW WORKING FORMULATION FOR GASTRIC CORROSIVE STRICTURE
Back to 2015 Annual Meeting Program
|

