|
Back to 2015 Annual Meeting Program
Outcomes After Completion Total Gastrectomy for Gastric Remnant Cancer
Etienne St-Louis*1, Stephen D. Gowing1, Mara L. Leimanis1, Pedram Mossallanejad2, Carmen L. Mueller1, Lorenzo E. Ferri1, 3
1General Surgery, McGill University, Montreal, QC, Canada; 2McGill University, Montreal, QC, Canada; 3Thoracic Surgery, McGill University, Montreal, QC, Canada
Gastric remnant cancer (GRC) arises in the residual gastric stump following partial gastrectomy. There is controversy about the safety and prognosis of completion total gastrectomy (GTC). We sought to describe our experience with this procedure and compare outcomes in patients undergoing CTG for GRC with patients undergoing primary total gastrectomy (PTG) for sporadic gastric cancer (SGC) in a high throughput tertiary care center.
A single institution, prospectively entered, clinical database of gastrectomy patients from 2005-2014 was retrospectively analyzed for demographic, surgical and clinical data as well as tumor pathology data and post-operative outcomes including complications and length of stay (LOS). Patients undergoing CTG were compared in these variables to patients undergoing PTG. Data is presented as median (range) and Chi-square, Fisher's exact and Wilcoxon rank sum tests were used to compare groups (* p<0.05).
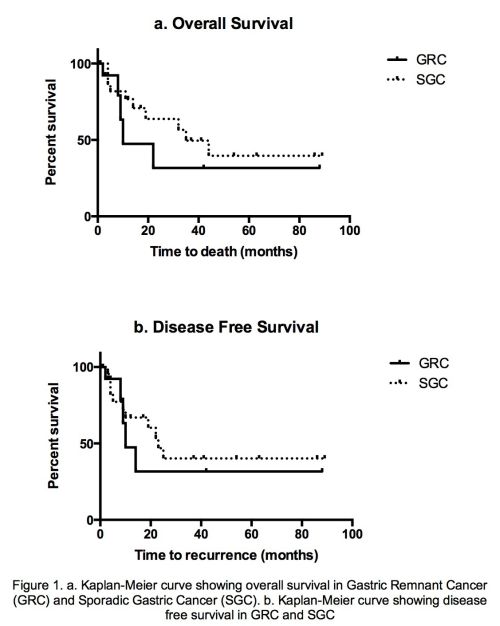
Out of 264 patients undergoing gastrectomy, we identified 37 who had non-palliative total gastrectomy for cancer (16 CTG, 33 PTG). Patient demographics were equivalent at baseline. There were no significant differences in operative or oncologic characteristics between CTG and PTG, pT≥4a (29% vs. 22% - NS) and pN≥1 (77% vs. 61% - NS), R0 resection rate (86% vs. 79% - NS), lymphadenectomy ≥D2 (64% vs. 87% - NS) or positive to negative lymph node (LN) ratio (0.1 (0.03-0.3) vs. 0.09 (0-0.65) - NS). However, median LN retrieval was significantly lower in CTG compared with PTG (14 (10-21) vs. 29 (20-48))*. CTG was associated with a slightly higher rate of overall complications (Clavien I-V) and reoperations (25% vs. 3%)* but this did not impact length of stay (8 (6-14) vs. 9 (7-18) days - NS) or in-hospital mortality (none in either group). There were no significant differences in median overall survival (10 (9-13) vs. 35 (14-56) months - NS), disease free survival (DFS) at 3 years (32% vs. 40% - NS) or overall survival (OS) at 3 years (32% vs. 50% - NS) - see figure.
Treating surgeons should recognize that although more technically challenging, completion total gastrectomy can be performed with equivalent post-operative and oncologic outcomes as primary total gastrectomy.
Back to 2015 Annual Meeting Program
|

