|
Back to 2015 Annual Meeting Program
the Impact of Adhesiolysis During Elective Abdominal Surgery on Quality of Life
Chema Strik*, Martijn W. Stommel, Richard P. Ten Broek, Harry Van Goor
Abdominal Surgery, Radboud University Medical Center, Nijmegen, Netherlands
Background
Patient-reported outcomes (PROs) encompass all areas of the patients' experience that can be measured such as quality of life. The outcome of quality of care for abdominal surgery has been traditionally reported in terms of morbidity and mortality. Due to developments in surgical technology and a decline in mortality from cancer, PROs are becoming an increasingly important aspect of abdominal surgery. The impact of adhesiolysis during abdominal surgery results in increased operative time and a longer and more complicated convalescence. Although a clear association between adhesiolysis, intraoperative adverse events and postoperative morbidity has been established, the impact of adhesiolysis on PROs after abdominal surgery has never been investigated.
Aim
To assess the impact of adhesiolysis and adhesiolysis-related complications on quality of life 6 months after surgery in patients undergoing elective abdominal surgery.
Methods
Design
Prospective cohort study, before surgery and six months after discharge patients were asked to complete the SF-36 questionnaire. Univariable and multivariable linear regression analyses were used to assess the impact of patient factors on the total score of the SF-36.
Settings
Tertiary referral university medical center
Participants
Patients participating in the LAPAD study, undergoing elective abdominal surgery
Results
518 (78%) out of 662 patients completed pre- and postoperative questionnaires. 319 (62%) patients required adhesiolysis during surgery. Overall pre- and postoperative quality of life did not significantly differ between patients requiring or not requiring adhesiolysis. (figure 1). Postoperatively, only physical functioning was significantly lower for patients requiring adhesiolysis (p 0.01). In the multivariable analysis, chronic abdominal pain (B -0.14; p <0.01), postoperative Clavien-Dindo grade 4 complications (B -0.15; p <0.01), concomitant pulmonary disease (B -0.06; p 0.04), age (-0.00; p 0.04) and readmissions within and after 30 days (B -0.06; p 0.01 and B -0.07; p <0.01) decreased quality of life 6 months after surgery the most (table 1). A higher preoperative SF-36 score (B 0.44; p <0.01) positively impacted quality of life after surgery.
Conclusion
Chronic abdominal pain and Clavien-Dindo grade 4 complications have a large negative impact on postoperative quality of life 6 months after surgery for patients undergoing elective abdominal surgery. Additionally, age, concomitant pulmonary disease and readmissions also show to negatively impact the quality of life of patients. Higher preoperative quality of life showed to be an independent protective factor for postoperative quality of life. The need for adhesiolysis during abdominal surgery does not directly impair quality of life of patients 6 months after surgery. These results can be used for improving patient counseling.
Table 1 Multivariable linear regression analysis for patient factors impacting the SF-36 score 6 months after surgery
| Patient factors | B | Lower limit 95% CI | Upper limit 95% CI | p value | | Age | -0.00 | -0.00 | 0.00 | 0.04 | | Comorbidity; pulmonary disease† | -0.06 | -0.11 | -0.00 | 0.04 | | Laparoscopic approach | 0.06 | 0.00 | 0.12 | 0.04 | | Anatomical site of operation; other‡ | -0.08 | -0.13 | -0.03 | ≤0.01 | | Adhesiolysis-related complications; serosal injury¥ | -0.04 | -0.08 | 0.01 | 0.10 | | Postoperative complication; Clavien-Dindo grade 4 | -0.15 | -0.25 | -0.05 | ≤0.01 | | Readmission; within 30 days after discharge | -0.06 | -0.11 | -0.02 | 0.01 | | Readmission; after 30 days after discharge | -0.07 | -0.12 | -0.03 | ≤0.01 | | Chronic postoperative abdominal pain 6 months after surgery‖ | -0.14 | -0.18 | -0.11 | ≤0.01 | | Preoperative SF-36 score | 0.44 | 0.36 | 0.51 | ≤0.01 |
Explanation special characters: †: comprising chronic obstructive pulmonary disease, asthma and emphysema; ‡: comprising retroperitoneal sarcoma, lymphatic and kidney resections, splenectomies and open abdominal aortic repair; ¥: defined as injury to the serosal and muscular layers of the bowel, without visualization of the bowel lumen or spillage of bowel content: ‖: defined as abdominal pain interfering with social activities or worse 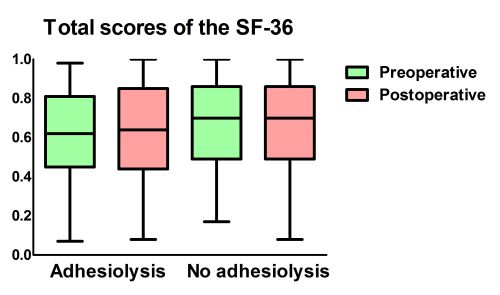
Back to 2015 Annual Meeting Program
|

