|


|
Back to 2014 Annual Meeting Posters Anatomo-Radiologic Study of the Vascularisation of the Pancreas Interrelated With Resective Surgery Edgardo Picardi*1,2, Veronica Macchi1, Andrea Porzionato1, Aldo Morra3, Carla Stecco1, Francesca Zingales2, Romeo Bardini2, Raffaele De Caro1 1Dep Molecular Medicine, Institute of Human Anatomy, Padova, Italy; 2General Surgery, Padova, Italy; 3Euganea Medica, Diagnostic centre, Padova, Italy
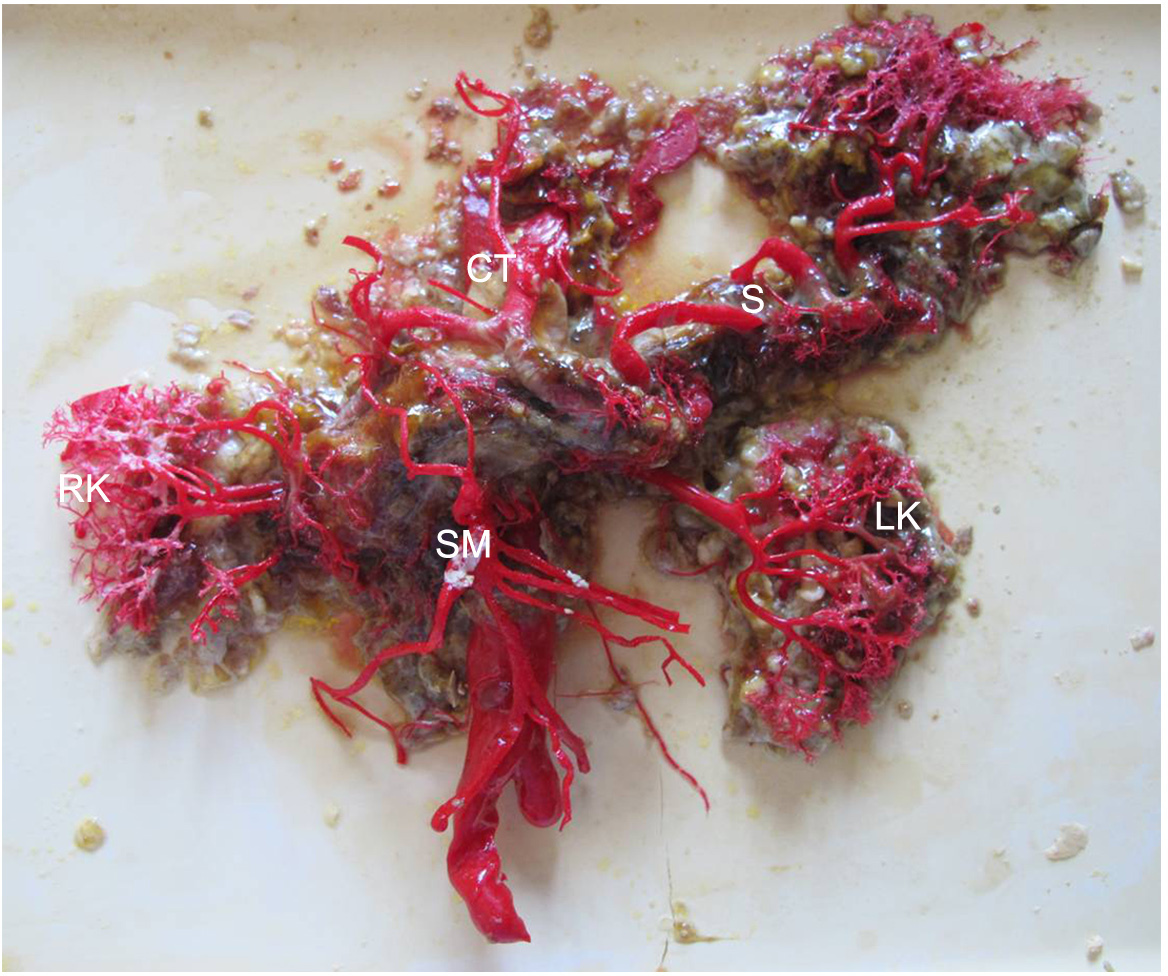
Postoperative pancreatic fistula is still regarded as a major complication. The aim of the present study was to describe the different patterns of the vascular architecture of the pancreas and to evaluate if they can predict the risk of postoperative complications after pancreatoduodenectomy (DCP). 9 specimens of duodenum, pancreas and spleen, were injected with acrylic resins to obtain vascular casts of the pancreas. 30 angiographies with computed tomography (CT angiography) of subjects without pancreatic pathology were analyzed to assess the depiction rate and to perform a detailed description (origin, calibre, course, anastomosis, variations) of: posterior superior pancreaticoduodenal artery (PDPS), anterior superior (PDAS), inferior pancreaticoduodenal (PDI), posterior inferior (PDPI), anterior inferior (PDAI), dorsal pancreatic (PD), magna (PM), transverse (PT) and caudal (PC). We have also analyzed thirteen pre-operative CT angiographies of patients who underwent DCP. At the level of the pancreatic neck a paucivascular area was appreciable in all vascular casts. The PT artery is the only artery, linking the cervicocephalic segment with the somatocaudal one, originating from PD artery in 26.9%, from superior mesenteric artery (AMS) in 19.2%, from splenic artery in 7.7%, from pancreaticduodenaljejunal trunk (PDJ) in 7.7%, from gastroduodenal artery, PM and PDPI in 3.8%. High risk vascular patterns of post-operative complications are: presence of a splenic artery with intrapancreatic course (33.3%), especially when combined with the absence of PT (44,4% vs 83,3% of cases with splenic artery with suprapancreatic course); presence of a PDI artery originating from the PDJ trunk (28.6%) or presence of PDAI and PDPI arteries arising from PDJ trunk (respectively 50% and 45.5%) or from first/second jejunal artery (11.1% and 18.2%); presence of PD artery originating from AMS (3.8%) (with focus on the distance between these vessels) or a PT originating from AMS (26.9%) which goes first on the right and then on the left side; presence of a right hepatic artery originating from AMS (7.7%), especially from the right side, and in combination with a gastroduodenal artery originating from an aberrant right hepatic artery (10.3%); presence of compensator circulations in patients with mesenteric or celiac arterial stenosis. At the level of the pancreatic neck the paucivascular area corresponds to an area of microcirculation of the parenchyma due to the absence of vessels with significant calibre. It can facilitate the execution of the resection of the pancreatic head, but it makes the body-tail stump vulnerable to postoperative ischemic insults. Great attention to the preoperative study of patients undergoing DCP should be paid to analyze in detail the individual vascular anatomy, through a close relationship between the surgeon and the radiologist. 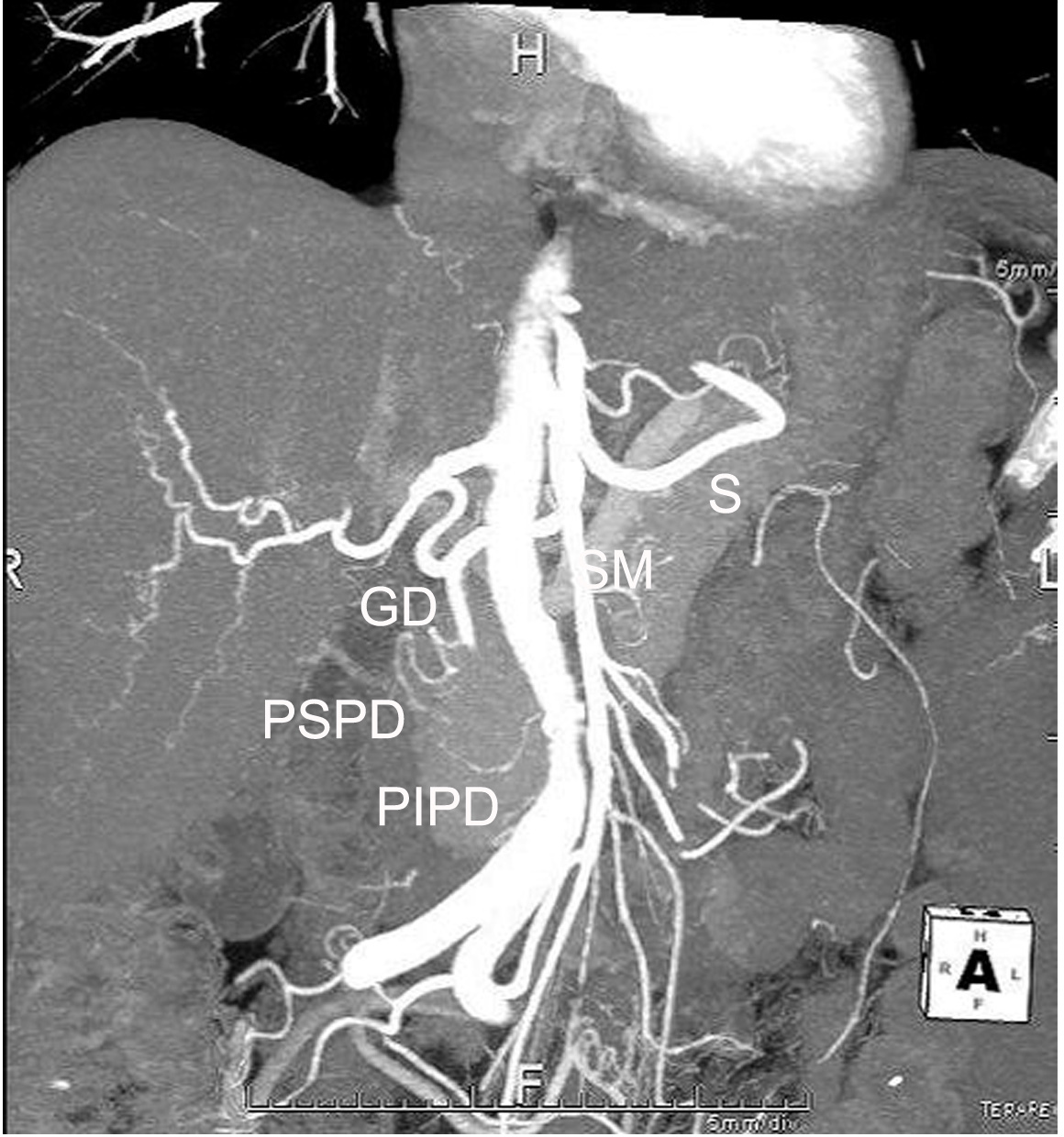 MIP reconstruction of a CT angiography, coronal view. SM mesenteric artery, S splenic artery, GD gastroduodenal artery, PSPD posterior superior pancreaticoduodenal artery, PIPD posterior inferior pancreaticoduodenal artery. Back to 2014 Annual Meeting Posters |
||||||||||
© 2026 Society for Surgery of the Alimentary Tract. All Rights Reserved. Read the Privacy Policy.