|
Back to 2014 Annual Meeting Posters
Repeated Re-Cycling of Aspirated Digestive Juices to Enzymatically Cleanse Feeding-Decompression Catheters and Return Previously Discarded Secretory Globulins
Gerald Moss*
Biomedical Engineering Department, Rensselaer Polytechnic Inst, White Plains, NY
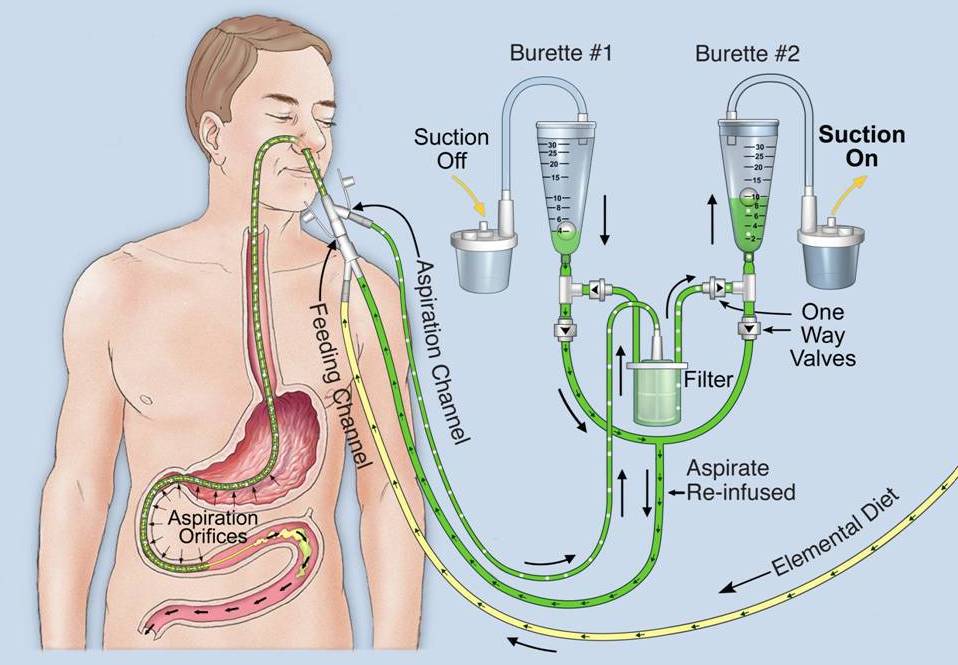
Combined enteral feeding plus decompression catheters are prone to proteinaceous clogging of both their suction and delivery channels, primarily the former. At the same time, proteolytic digestive secretions are removed and discarded by these devices. The aspirate should be re-fed to enzymatically cleanse the catheter's channels. This fluid also contains secretory globulins that should be salvaged to protect the vulnerable patient against invasion by colonic organisms.
The flow of aspirate is usually too sluggish to effectively flush the catheter. The volume of aspirate recycling can be increased by deliberate production of a "controlled leak" between the distal ends of the feeding and suction channels, analogous to an A-V fistula. This increased flow will be totally re-fed, and does not affect the volume lost from the patient.
A Moss® feeding - decompression catheter was modified by micro-drilling an ~0.001" diameter passage between the distal feeding and aspiration channels. This increased the volume of aspirate to be re-cycled for flushing ten-fold, from ~1.5 ml to ~15 ml. This approximately half-filled the 30 ml collection chambers during each 30 second cycle.
A pair of collection burettes were positioned five feet above the patient. Continuous suction was applied alternately, at 30 second intervals, to one or the other of the burettes. These chambers were connect by one-way valves to the catheter's aspiration and feeding channels.
The filtered aspirate was directed for 30 seconds by these one-way valves to the burette on suction for collection and degassing, as well as overflow if necessary to avoid overfeeding. The valves simultaneously directed the flow by gravity of degassed aspirate, which had been collected the previous 30 seconds in the burette now off suction. This joined the continuous 3,000 ml/day flow of elemental diet into the feeding channel.
When total inflow (feedings plus re-fed aspirate) exceeded peristaltic outflow from the duodenal feeding site, the volume rose in the collection burette on suction. Any excess greater than 30 ml overflowed, to be permanently discarded before it could cause local distention and the detrimental consequences of overfeeding.
In our experience, 3 - 4 liters/day of aspirated digestive secretions were removed and degassed by this automatic system. The volume of permanently removed fluid was only ~200 ml/day following resective thoraco- and/or abdominal surgery, without occurrence of overfeeding.
The degree of expected protection afforded against catheter clogging has not yet been objectively determined.

Back to 2014 Annual Meeting Posters
|