|
|
Back to 2014 Annual Meeting Posters
Prediction of Islet Yield in Patients Undergoing Total Pancreatectomy With Islet Autotransplantation (Tpiat) for Non-Calcific Chronic Pancreatitis (NCCP) Using Contrast Enhanced MRI and Secretin Stimulated MRCP (sMRCP)
Guru Trikudanathan*1, Satish Munigala2, Sidney Walker3, Ahmad Malli4, a. Balamurugan5,6, Joshua J. Wilhelm5,6, Timothy L. Pruett5, TY Dunn5, Greg Beilman5, David Sutherland5, Mustafa a. Arain1, Shawn Mallery1, Rajeev Attam1, Martin L. Freeman1, Melena Bellin6
1Gastroenterology, Univerisity of Minnesota, Minneapolis, MN; 2Gastroenterology, St Louis University School of Medicine, St Louis, MN; 3Radiology, Center for Diagnostic Imaging, St Louis, MN; 4Internal Medicine, University of Minnesota, Minneapolis, MN; 5Surgery, University of Minnesota, Minneapolis, MN; 6Endocrinology, The Schulze Diabetes Institute, Minneapolis, MN
Background and Aim:
Insulin independence after TPIAT is impacted by the number and quality of islets transplanted. Contrast enhanced MRI with sMRCP offers a safe and non-invasive modality to diagnose chronic pancreatitis. In this study, we aimed to correlate the islet yield with the parenchymal imaging findings on MRI and ductal changes on sMRCP within the subpopulation of patients undergoing TPIAT for non-calcific chronic pancreatitis (NCCP).
Methods:
Adults patients with NCCP undergoing TPIAT, between 2008 and 2013 were included if they had a contrast enhanced MRI with sMRCP within a year of surgery. An experienced radiologist blinded to islet yield data following TPIAT determined the presence or absence of qualitative MRI features including atrophy (defined as antero-posterior (AP) diameter <20mm), main pancreatic duct (MPD) irregularity, MPD stenosis, MPD dilation, presence of side branches, and abnormal duodenal filling after secretin injection. Chi square analysis was performed to determine if presence or absence of individual features was associated with high islet yield (>300,000 IEQ or >5,000 IEQ/kg). In addition, AP diameter (as a continuous variable) was correlated with total islet equivalents isolated (IEQ), islet equivalents per kilogram (IEQ/Kg) and digestive tissue volume in univariate linear regression and a multivariate regression model controlling for demographic variables (age, sex, history of smoking, and body mass index). Continuous variables are expressed in mean ± standard deviation (SD).
Results:
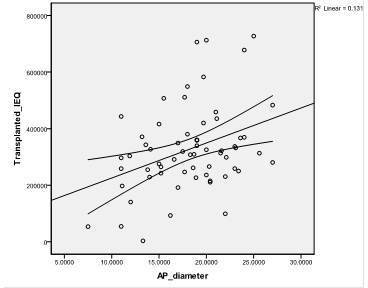
63 patients [54 females (85%), mean age 37.7±11.7] with NCCP with pre TPIAT contrast enhanced MRI with sMRCP were included in this study. Patients had a mean islet yield at procurement of 327,506± 151,641 islet equivalents (IEQ) and 4,688± 2,108 IEQ/kg body weight (IEQ/kg). Presence or absence of any single MRI feature (atrophy or ductal changes) did not adequately predict high islet yield. However, AP diameter significantly correlated with total IEQ (r=0.36, p=0.004, figure 1) and IEQ/kg (r=0.32, p=0.01), but also with higher digest tissue volume (r=0.33, p=0.008); these findings remained significant after taking into account patient age, sex, smoking status, and BMI.
Conclusion:
In patients with NCCP, greater AP diameter on contrast enhanced MRI/sMRCP was associated with higher islet yield. Because islet mass transplanted is a major determinant of later insulin use, these results suggest that MRI/sMRCP may offer an additional tool to aid in counseling prospective TPIAT patients with NCCP on diabetes risk after surgery.
 Figure 1: Total IEQ vs AP diameter
Back to 2014 Annual Meeting Posters
|