|
Back to 2014 Annual Meeting Posters
Excision and Revision of Ileal Pouch-Anal Anastomosis: Insights From 308 NSQIP Cases
Andrea M. Stroud*1, Corey a. Siegel2, Stefan D. Holubar1
1Colon & Rectal Surgery, Dartmouth-Hitchcock Medical Center, Lebanon, NH; 2Gastroenterology & Hepatology, Dartmouth-Hitchcock Medical Center, Lebanon, NH
PURPOSE: Ileal pouch-anal anastomosis (IPAA) is the gold-standard surgical treatment for medically refractory ulcerative colitis. However, small proportions of patients will develop complications requiring ileal pouch excision or revision. Currently only single institution series inform decision-making surrounding these uncommon procedures. We aimed to describe differences in short-term post-operative outcomes associated with pouch excision or revision procedures using a large national database.
METHODS: Using the American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) database from 2005-2011, we identified all patients who underwent ileal pouch excision (PEx) or pouch revision via a combined abdominoperineal approach (AP) or perineal only approach (PR) with Current Procedural Terminology (CPT) codes. We compared baseline characteristics, diagnoses, and short-term outcomes across these procedures using simple descriptive statistics.
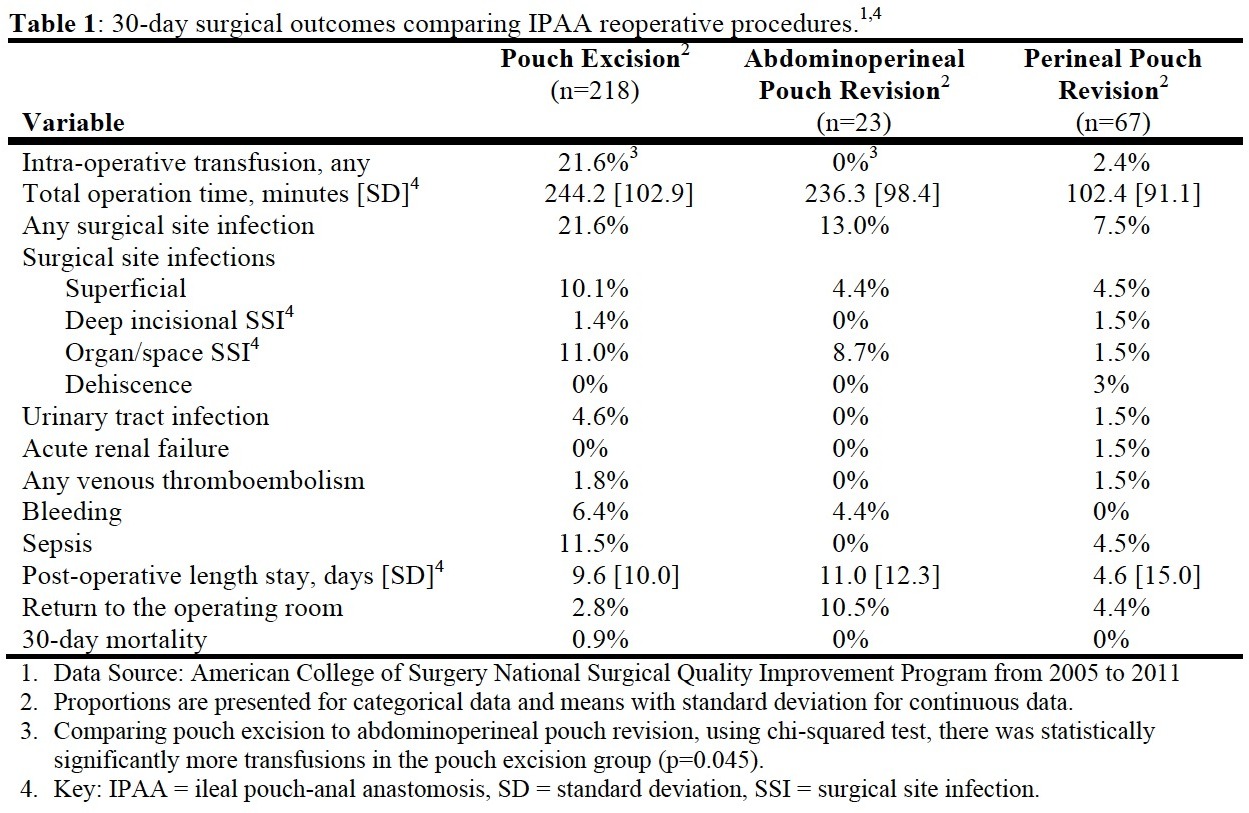
RESULTS: Of 348,221 colorectal operations, we identified 308 cases of pouch excision or revision: 218 excisions and 90 revisions (23 AP, 67 PR). AP patients were younger (36.4 vs. 47.0 (PEx) and 42.2 (PR) years, p=0.003), more likely to be male (60.9% vs. 54.6% (PEx) and 35.8% (PR), p=0.017), and of similar BMI (24.5 kg/m2). We found no difference between the groups in regards to other pre-operative characteristics including chronic steroid use, chemotherapy, radiation therapy, weight loss, transfusion, sepsis, prior operation within 30-days, creatinine, or albumin. Pre-operative diagnoses were heterogeneous and commonly missing; just over half (53.5%) had a specific diagnosis reported. The most common diagnoses were fistula/infection, chronic ulcerative colitis, and Crohn's disease. Chronic ulcerative colitis was the most common diagnosis in both PEx (11.5%) and AP (17.4%), while pouch-vaginal fistulas was the most common diagnosis in the PR (19.4%) patients. Thirty-day outcomes are presented in Table 1. PR patients had shorter operative times (102 vs. 244 (PEx) and 236 (AP) minutes, p<0.001), fewer surgical site infections (7.5% vs. 21.6% (PEx) and 13% (AP), p=0.03), and shorter length of stay (4.6 vs. 9.6 (PEx) and 11.0 (AP) days, p=0.005). When comparing PEx to only AP, the only statistically significant difference in short-term outcomes was increased transfusions in the PEx patients (21.6% vs. 0% (AP), p=0.045). The only 2 deaths occurred in the PEx group.
CONCLUSIONS: This national cohort represents one of the largest series of reoperative procedures for failed or failing IPAA reported to date. Pouch excision and revision procedures are rare, have acceptable operative morbidity, and low operative mortality. These data can help inform surgeons and gastroenterologists when counseling patients with respect to complications related to IPAA and expected outcomes of reoperative procedures.

Back to 2014 Annual Meeting Posters
|