|
Back to 2014 Annual Meeting Abstracts
Short-Term Oncologic Outcomes Are Superior Following Laparoscopic Versus Open Low Anterior Resection for Rectal Cancer: Results From the National Cancer Database
Daniel P. Nussbaum*, Paul J. Speicher, Asvin M. Ganapathi, Brian R. Englum, Jeffrey E. Keenan, Christopher R. Mantyh, John Migaly
Surgery, Duke University Medical Center, Durham, NC
BACKGROUND: While laparoscopy has emerged as a standard technique for patients undergoing colorectal surgery, there is ongoing debate regarding the oncologic equivalence of laparoscopic compared to open low anterior resection (LAR) for rectal cancer. Clinical trials are underway to evaluate this question (ACOSOG-Z6051); however, final results will not be available for some time. In the interim, the purpose of this study is to evaluate the short-term oncologic outcomes for patients undergoing laparoscopic versus open LAR.
METHODS: The National Cancer Database (NCDB) was queried to identify patients undergoing LAR for rectal cancer between 2010-2011. Subjects were stratified by laparoscopic (LLAR) versus open (OLAR) technique. Perioperative variables were compared between groups, and subjects were then propensity matched using a 1:1 nearest-neighbor algorithm to adjust for bias at the level of treatment decision. Finally, short-term outcomes were compared between groups.
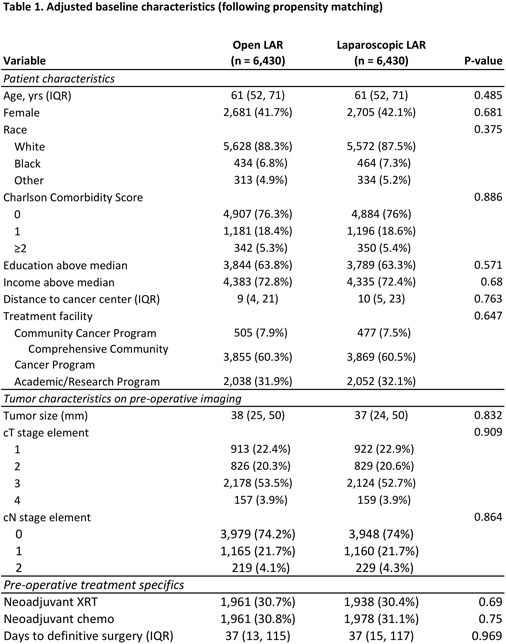
RESULTS: A total of 18,765 patients underwent LAR for rectal cancer, of which 6,430 (34.3%) were performed laparoscopically. Patients who underwent LLAR were slightly younger (61 vs. 62 years, p<0.001). Those undergoing LLAR were more likely to have pre-operative T-stage 1/2 than T-stage 3/4 disease (p<0.001) and were less likely to have radiographic evidence of nodal involvement (p<0.001); thus, these patients were also less likely to have received neoadjuvant chemoradiation therapy (p<0.001). After propensity matching, however, all baseline variables between groups were highly similar, including pre-operative stage, radiographic tumor characteristics, and use of neoadjuvant therapy (Table 1).
Patients undergoing LLAR were more likely to have both gross (97.8 vs. 96.5%, p<0.001) and microscopic (97.1 vs. 96.6%, p<0.001) negative margins following surgical resection. Moreover, circumferential margins of at least 1mm were achieved more frequently in patients undergoing LLAR (94.3 vs. 92.2%, p<0.001). There was no difference in median number of regional lymph nodes obtained (15 vs. 15). Patients undergoing LLAR had a shorter hospital length of stay (5 vs. 6 days, p<0.001) without a corresponding increase in 30-day readmission rates (6 vs. 7%, p=0.02). Overall, there was no difference in 30-day mortality (1.3 vs. 1.7%, p=0.06).
CONCLUSIONS: Laparoscopic low anterior resection is a safe alternative to open surgery for patients with rectal cancer, with meaningful reductions in hospital length of stay. Furthermore, LLAR may also result in superior short-term oncologic outcomes as measured via surrogate pathologic endpoints in the NCDB. While these results support the increasing use of laparoscopy in colorectal surgery, further data are necessary to assess long-term outcomes. The final results of ACOSOG-Z6051 are eagerly awaited.

Back to 2014 Annual Meeting Abstracts
|