|
Back to 2014 Annual Meeting Abstracts
Survival Implications of Non-Regional Lymph Node Involvement on Staging PET/CT for Esophageal Adenocarcinoma
Michal J. Lada*, Michelle S. Han, Andreas Tschoner, Christian G. Peyre, Carolyn E. Jones, Thomas J. Watson, Jeffrey H. Peters
Surgery, University of Rochester Medical Center, Rochester, NY
Objectives: With the advent of routine staging PET/CT in the evaluation of esophageal adenocarcinoma (EAC), PET-positive non-regional lymph nodes (NRLN) are commonly encountered. These have traditionally been grouped with distant organ metastases although the clinical significance of PET-positive lymph nodes outside the boundaries of standard resection margins is unknown, particularly in the era of routine neoadjuvant chemoradiotherapy. Our aim was to assess the prevalence, clinical implications and survival outcomes of patients with NRLN on pre-treatment clinical staging.
Methods: The study population consisted of 310 patients with EAC evaluated between 2005 and 2012. The mean age was 65±0.6 years and 86% were male. All had pre-treatment staging PET/CT imaging. PET-positive lymph nodes (LN) were defined as SUVmax >1.5. Regional lymph nodes (RLN) were defined as infra-carinal paraesophageal, left gastric, lesser curve or celiac lymph nodes. NRLN were defined as those outside of these resection fields; namely, above the carina and below the celiac axis. Survival was estimated via the Kaplan-Meier method.
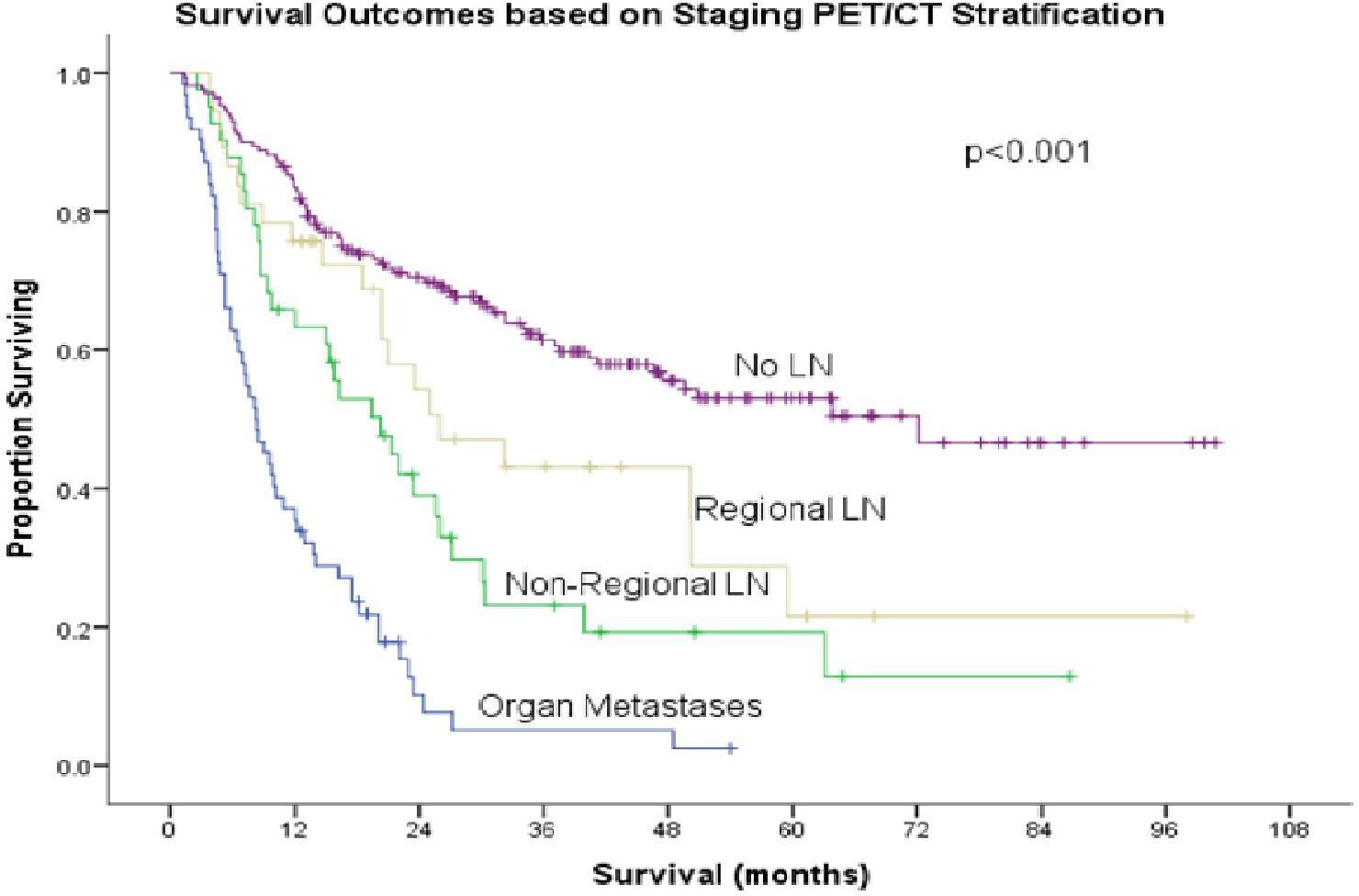
Results: Hypermetabolic lymph nodes were identified in 26% (80/310) of the patients, of which 47% (38/80) had RLN and 53% (42/80) had NRLN. Distant organ metastases were noted in 18% (55/310) and no metastases in 56% (175/310) of the patients. Esophagectomy was performed in 61% (188) of the patients of which 60% (112) received neoadjuvant therapy. Five-year survival (KM) was 50% in patients with no evidence of metastases, 22% in patients with RLN alone, 12% in those with NRLN, and 0% in patients with distant organ metastases. Patients with NRLN had significantly better 5-year survival than those with organ metastases (p<0.001, Figure). Median survival in patients with NRLN s/p neoadjuvant therapy and esophagectomy was significantly longer than in patients with solid organ metastases (17.9 vs. 8.2 months, p<0.001).
Conclusions: Routine use of PET/CT staging identifies non-regional lymph node disease in half of patients with clinically positive nodes and almost 15% of all patients. Although long-term survival is not as good as patients who are clinically node negative or with regional nodes, combined neoadjuvant therapy and esophagectomy result in improved survival over patients with solid organ metastases.
Back to 2014 Annual Meeting Abstracts
|